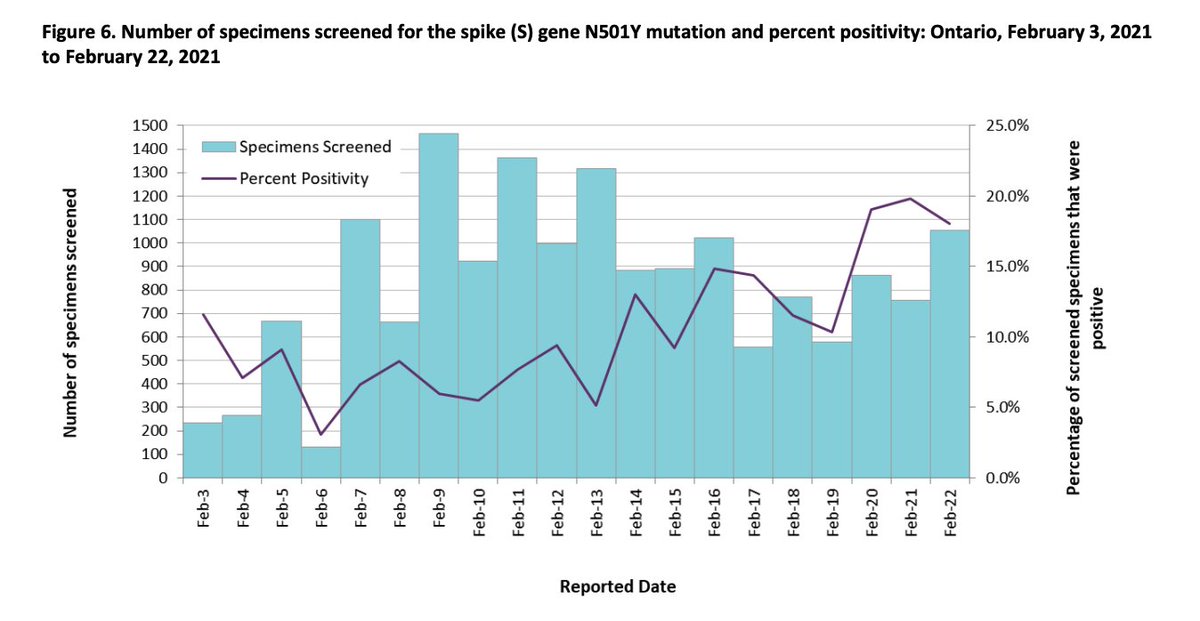
Ontario is screening all positive COVID cases for the N501Y mutation present in B.1.1.7 and the trend does not look good. Total case counts (and so deaths) will certainly be on the rise again soon as B.1.1.7 begins to dominate. 😢
Ontario is screening all positive COVID cases for the N501Y mutation present in B.1.1.7 and the trend does not look good. Total case counts (and so deaths) will certainly be on the rise again soon as B.1.1.7 begins to dominate. 😢
8 months ago: “Masks won’t help you. They need to be saved for health care workers - they’re the ones who need infection control”
Today: “Frequent rapid testing isn’t helpful for you. It only helps celebrities - they’re the ones who need to prevent outbreaks” https://twitter.com/RapidTests/status/1367244825251082245
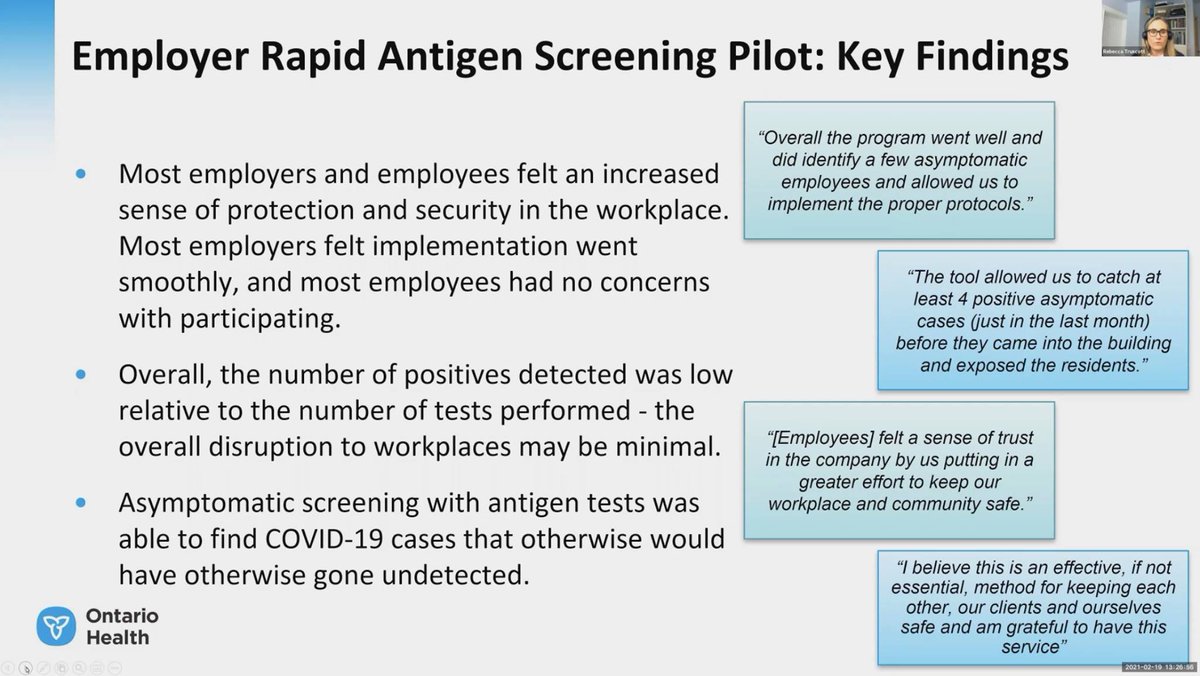
Rapid antigen tests working to reduce the spread of COVID in Ontario workplaces under Public Health Ontario screening program:
From https://www.ontariohealth.ca/COVID-19/Health-System-Response-Resources#panbio and https://www.youtube.com/watch?v=XkcK5pbCAd4
@RapidTests @TestandTraceCa @michaelmina_lab
Thank you @LisaBarrettID for your vision and drive-against-the-grain in pop-up rapid COVID screening! You are an inspiration across Canada and are now having great influence on screening in Ontario! https://www.dal.ca/news/2021/02/10/how-a-dal-doctor-has-taken-on-doubters-to-become-a-leading-voice.html
/cc @michaelmina_lab @TestandTraceCa
In computer science we make off by one errors. In microbiology I apparently make off by 10,000x errors! 😂
I diluted my DNA control by 100,000x when it should have been 1,000,000,000x to get down to a “reasonable” 6,000 copies of DNA per μl.
Wow, so prescient. “If you need to be right before you move, you will never win.” https://twitter.com/jkwan_md/status/1239312976198451201
This is huge. US joins Europe in empowering individuals to cheaply, easily and effectively screen for COVID at home.
How long will it take for Canada to follow? Will all antigen test manufacturing capacity be absorbed by the US now? https://twitter.com/michaelmina_lab/status/1377454976885219330
I think I’m starting to feel what punch card programming must of felt like.
Each iteration takes me 30 min of careful planning, 20 min to carefully formulate the instructions in the bizarre way the machine understands, an hour for the machine to follow my instructions, and…
then I spend hours pouring over the output trying to understand what the heck was going on inside the machine and how I’ll tweak my program next time.
But in this case, the machinery is biology (eg. Taq DNA Polymerase enzyme doing PCR experiments).
It’s super tedious but hella gratifying when stuff works! Makes me wish I was either coding computers in the 70s or hacking life in 2040 😁
Highly scaled serial screening programs like this could make the difference between Rt>1 (lockdowns) and Rt<1 (re-opening). Can we get to >10% of the population screening 2-3 times a week?
#StaySafeScreen @TestandTraceCa @michaelmina_lab https://twitter.com/iainklugman/status/1381627171140173825
I’m so grateful to @ianklugman, @communitech and the government of Canada for making this happen!
@VicLeungIDdoc Self-screening is what we’re doing with https://staysafescreen.ca and initial indications are that it’s working well! Essential business owners are overjoyed to be able to have their staff self-screen onsite.
@VicLeungIDdoc “In the UK, screening showed lower sensitivity when tests were performed by testers who were not health care workers than when they were performed by health care workers;however,”…
@VicLeungIDdoc “the discrepancy disappeared over a 2-week period, which suggests that workers who are not trained in health care can be taught with experience to adequately perform swabs.”
@VicLeungIDdoc The claim that COVID testing can’t be done by regular people will go down with “masks aren’t needed or only protect others” and “transmissions isn’t airborne” as the most deadly ideas of this pandemic.
Millions of secondary school students in England are doing COVID rapid antigen screening at home twice a week. Why them and not you?
https://www.bbc.com/news/health-56750460
Malaria continues to be a huge health crisis in Africa, even greater than COVID. An effective vaccine is incredibly good news! https://twitter.com/paulg/status/1385538759266086912
Sheesh, I can’t believe we still haven’t taken this to heart! People continuously come to the #StaySafeScreen bus expecting to have their nasal cavity abused, so many more would come if that wasn’t the expectation. https://x.com/RickByers/status/1243150948815581186
AZ Dose #1 - last Tuesday when it first became available in Ontario to 40+.

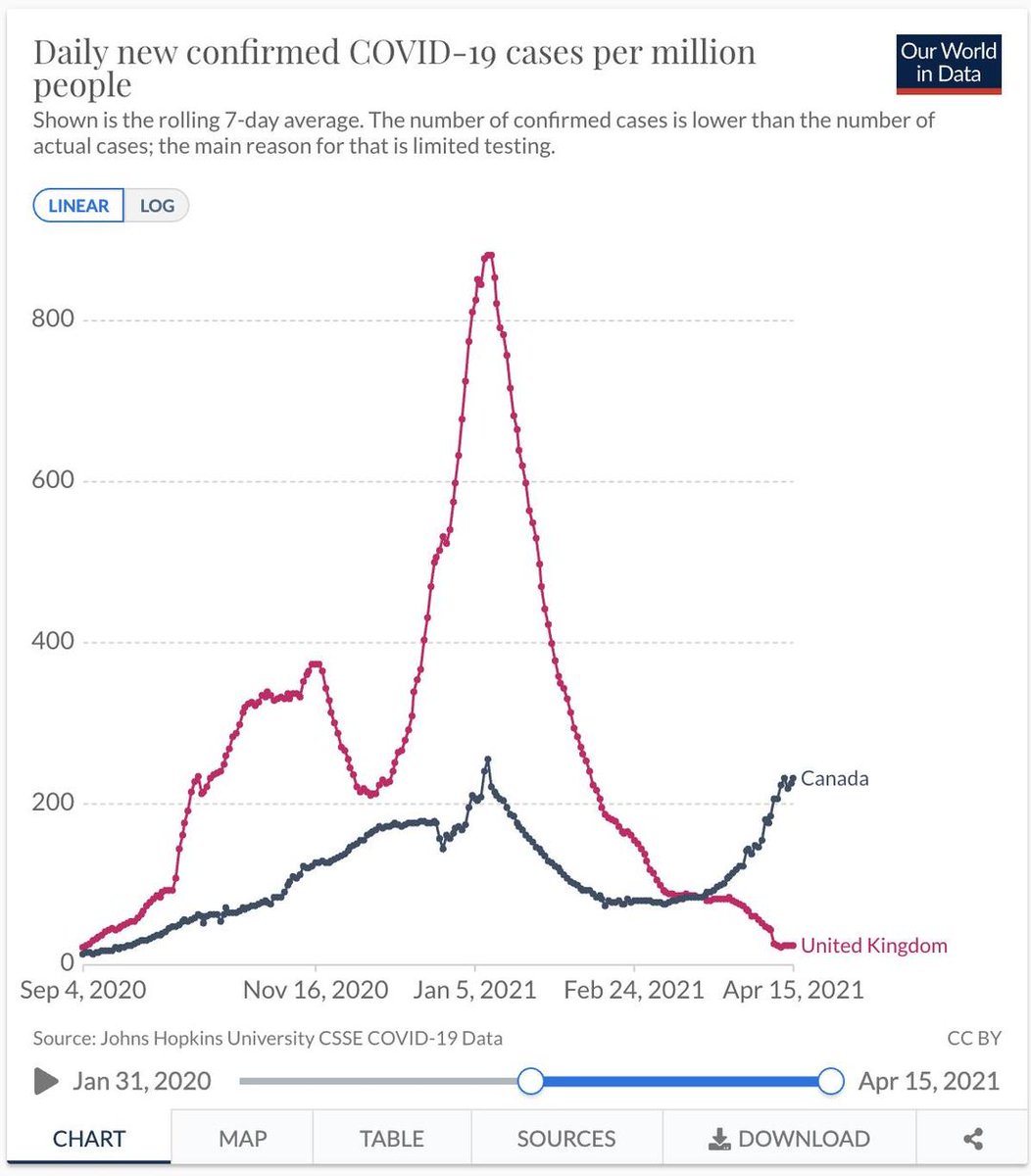
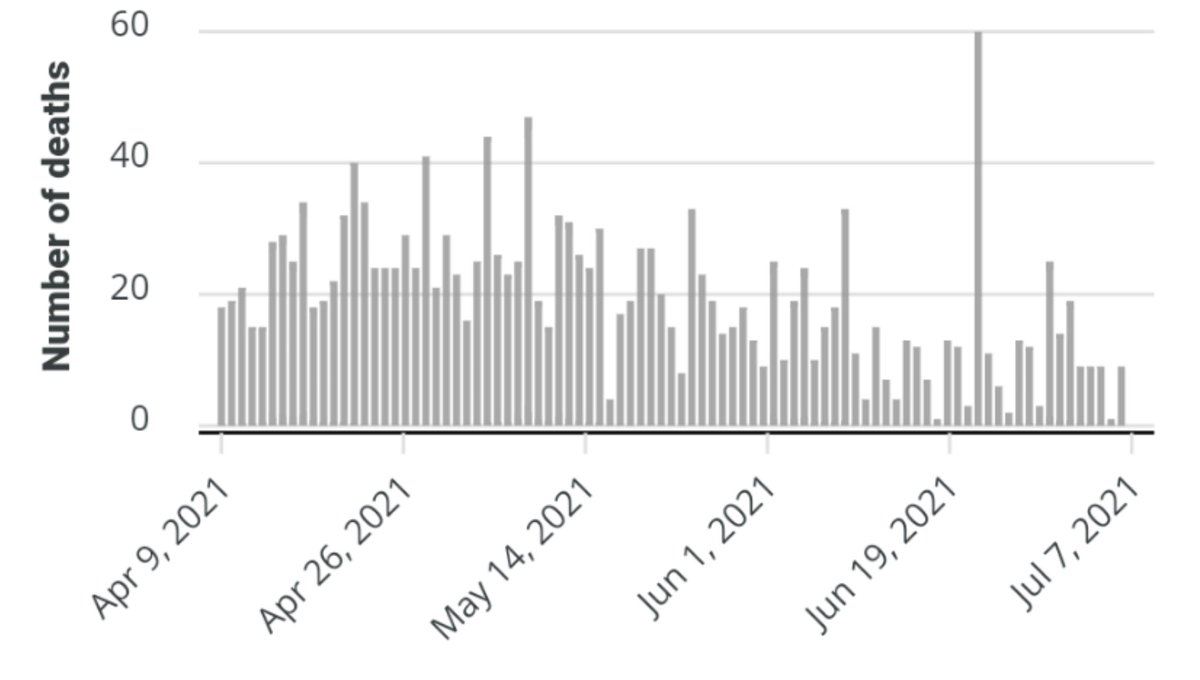
Might this difference in epi curves have anything to do with the 25,000 infection chains broken by rapid at-home antigen testing in England?
https://www.facebook.com/rick.byers/posts/10159567287421514
More coverage of the #StaySafeScreen rapid COVID antigen screening program in Waterloo region:
https://www.therecord.com/news/waterloo-region/2021/04/25/waterloo-region-businesses-feel-relieved-to-have-access-to-rapid-covid-testing.html
To keep from spamming my web followers with COVID tweets and my COVID followers with web tweets, I’m splitting my account. Follow @RickByersLab for COVID (but I’ll retweet for a couple weeks).
Free, comfortable and effective COVID-19 antigen screening on the #StaySafeScreen bus. Results texted to you in about 15 minutes! https://staysafescreen.ca/

By the way, this video is taken on my kitchen table. Why don’t you have these at home in your kitchen yet?
If millions of English high-school students and government employees are using them at home twice a week, surely you could too?
One business owner, nearly in tears, picking up their free #StaySafeScreen kits: “Every day I’ve woken up wondering if today would be they day I have an outbreak among my staff. Now I finally have a powerful tool to help avoid that.”
Love seeing the kits piled high, ready to be picked up. Each group of ~40 boxes represents one COVID transmission chain being broken. https://x.com/MusicalLives/status/1384617436201115660
@cat10086338 @RegionofHalton @HaltonHlthcare @OakvilleChamber @Communitech Here’s a photo of my Grade 9 son instructing someone on the #StaySafeScreen bus to self-swab. If millions of high-school students in England can self-swab at home, then I’m pretty sure Ontarians are up for it too! https://www.bbc.com/news/health-56750460

In the US now, anyone can buy one of these at a pharmacy and do an antigen screen at home. It’s painless and easy! How long will it take for Canada to follow this?
https://youtu.be/baQQfoX-JXo
As a “rich white dude” who has been testing myself and family for COVID at home regularly for the past year, I couldn’t agree more! The inequity is awful!
Get kits, get screened, twice a week, every week! #StaySafeScreen https://x.com/michaelmina_lab/status/1381827160390963203
Good coverage of the #StaySafeScreen program to distribute rapid antigen COVID screening kits to small businesses to self-administer onsite.
Also includes self-swabbing buses staffed by an army of volunteers like me! Free results in 15 min.
https://kitchener.ctvnews.ca/a-real-tool-that-will-have-a-real-impact-asymptomatic-testing-helping-small-businesses-1.5400334
In England rapid home COVID tests “detected over 120,000 positive cases that would not have been discovered otherwise”. Will the US follow England even before Canada does?
https://www.forbes.com/sites/williamhaseltine/2021/04/08/rapid-home-testing-if-the-uk-can-do-it-why-cant-we/
@COVIDSciOntario what are your thoughts on serial antigen screening as a tool to reduce community transmission? Have you reviewed, for example, https://pubmed.ncbi.nlm.nih.gov/33219112/ and https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00425-6/fulltext ?
These stories should no longer be a surprise. We’ve heard similar stories from around the world for many months. Rapid tests work to prevent and contain outbreaks! https://x.com/MichaelSchwandt/status/1388146533292417030
http://StaySafeScreen.ca starting to get national recognition, including from our PM. I hope the model will scale rapidly across Canada! https://x.com/JustinTrudeau/status/1389375447817916417
England is experimenting with allowing close contacts of COVID-19 individuals to replace isolation with daily rapid antigen testing. The results will be fascinating to see. Maybe not just a “red light” test anymore @michaelmina_lab? https://www.gov.uk/government/news/government-to-launch-40000-person-daily-contact-testing-study
Yes 2 is better than 1. But 2×1 looks pretty clearly better than 1×2 in most cases!
Similarly many people getting frequent lower-sensitivity antigen tests is better for containment then a few people occasionally getting highly-sensitive PCR tests.
Hard for many to reason about! https://x.com/jkwan_md/status/1389407379352137728
A compelling argument for rapid antigen testing and an inspiring story of a group deploying them at scale in Monterey, CA. https://x.com/sameerucla/status/1387907684473745418
I love the detective analogy. PCR is like checking everyone’s fingerprints, while antigen screening is having people be on the lookout for the description of a suspect (who can later have their fingerprints checked).
About 250 COVID transmission chains broken in the current wave in Nova Scotia thanks to rapid testing. These are asymptomatic people who would likely be unknowingly spreading the virus to others if it weren’t for rapid testing. https://x.com/LisaBarrettID/status/1389909284507561984
Great stories from @GregDurocher about what small business owners say it means to them to be empowered with rapid COVID screening: https://www.youtube.com/watch?v=lg_W2wzZr24&t=668s
“With the success of the StaySafe Rapid Testing Pilot in Waterloo Region, expanding rapid testing to small and medium-sized businesses across the province will help keep people working and safe”
https://news.ontario.ca/en/release/1000082/ontario-expands-covid-19-rapid-testing-across-province
“The root of the CDC’s behavior was simple: fear. They didn’t want to take any action for which they might later be blamed”.
From the book “The premonition”. Pretty much sums up much of the pandemic response. 😥 Fear of taking the wrong action is greater than fear of inaction.
In tech we know this mental disease well and how it breeds mediocrity if left unchecked. To combat it we have a “bias to action” and “blame-free post mortem culture”. Nobody is punished for making mistakes, only for failing to learn from them.
But then, in tech we aren’t charged with keeping millions of people
alive and healthy. I can’t imagine what that burden of responsibility does to one’s confidence or risk tolerance.
“Justin Trudeau gave credit to the StaySafe project in announcing the rapid testing expansion Friday. ‘Cases have been found in asymptomatic people who had no idea they were positive, but because of the test result, were then able to isolate to prevent transmission’ Trudeau said” https://x.com/btaplatt/status/1391114568831840261
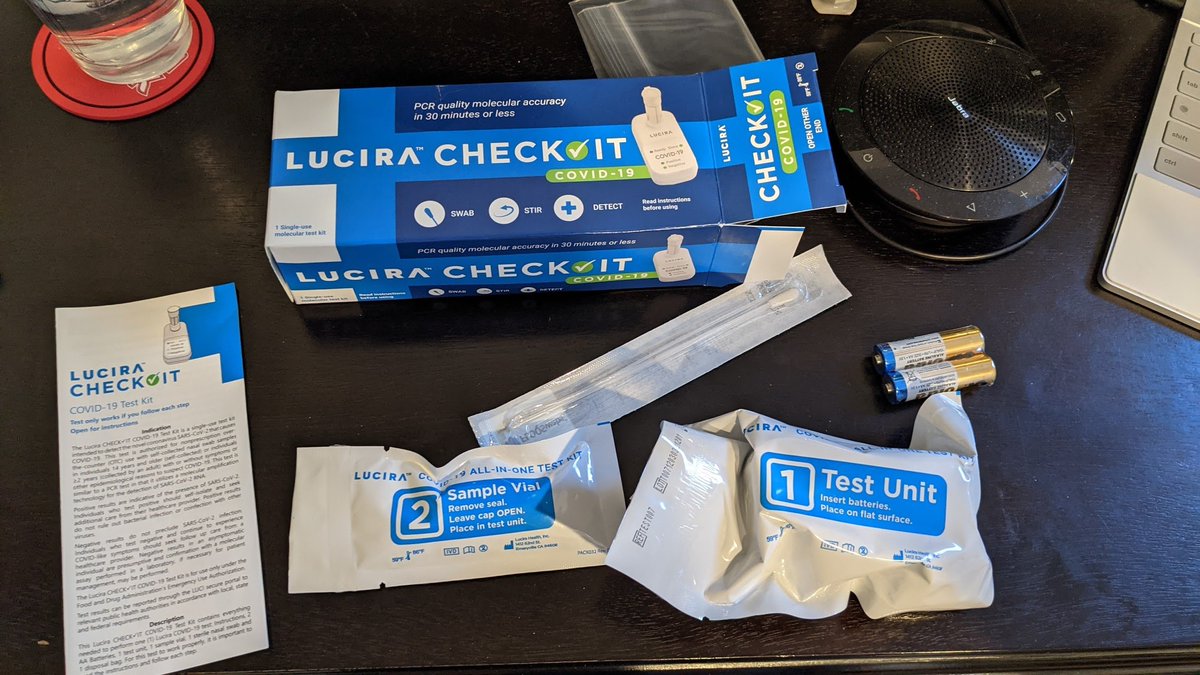
Received my Lucira Check-it home PCR-quality COVID test today for $75. I’ll be using this (instead of my $12,000 PCR machine) to check any positive antigen test results I get.
Antigen tests are awesome! But at 2 in 1,000 false positives, you need a pragmatic plan to validate!
Me a year ago: “Is there any good reason why the scale of consumer electronics manufacturing won’t be brought to bear on viral diagnostics, leading to devices being as common in pharmacies, offices and eventually homes as laser printers are today?“
https://rickbyers.medium.com/the-dawn-of-personal-biotech-cb0af0d52e4c
Every high school student in England has been testing themselves for COVID at home twice a week for the past couple months.
Big surprise, it appears to work in Canada too! 🙂 https://t.co/XHEanbRxiA
It’s 6 months later and the evidence just keeps mounting that @michaelmina_lab was right. How long before we’re all-in on home rapid testing?
Will we get enough experience with it to be ready to jump quickly at the start of the next pandemic? Or will we debate for a year again? https://x.com/michaelmina_lab/status/1328873625894719489
“Vaccine hesitancy and lottery enthusiasm are two sides of the same disregard for statistics. How better to reach people unswayed by expert advice on what is statistically likely to serve their interests than to offer a minuscule chance at $100 million?” https://x.com/NathanStall/status/1393242477893672961
Alright Canada, we’ve got a shot at >90%!🏃♀️💉
Let’s show the world that Canadians respect Science, understand probabilities, and care about the health of our fellow citizens! https://x.com/DavidColetto/status/1393893134069866500
“It’s a story of Canadian officialdom’s instinct for caution and over-regulation, rather than moving with the speed, urgency and innovation that a national emergency requires”
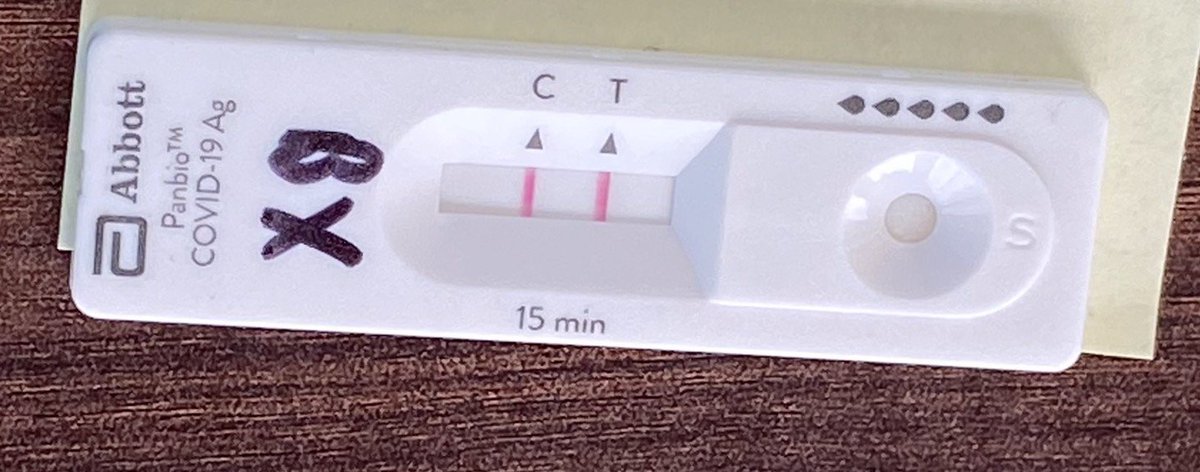
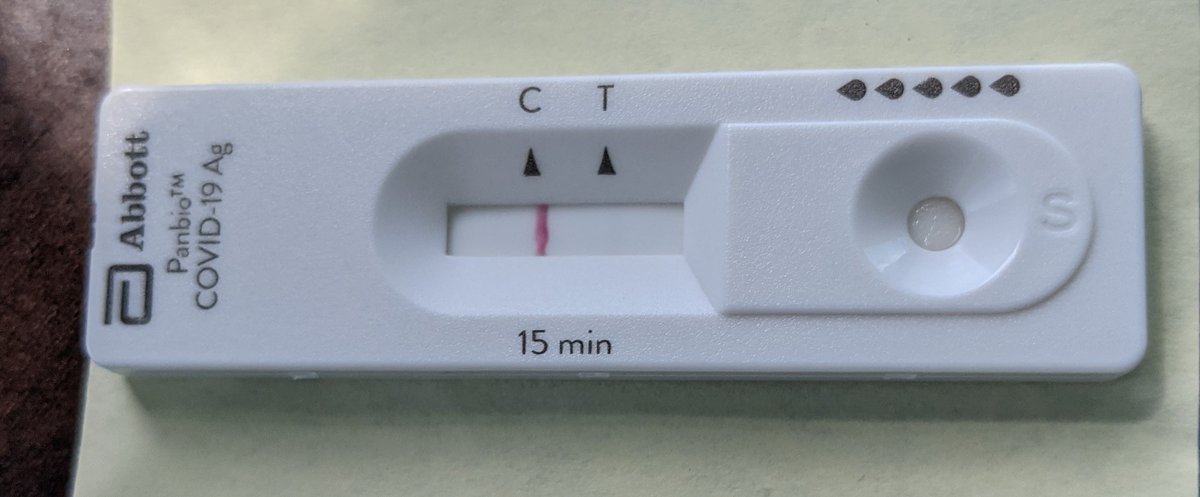
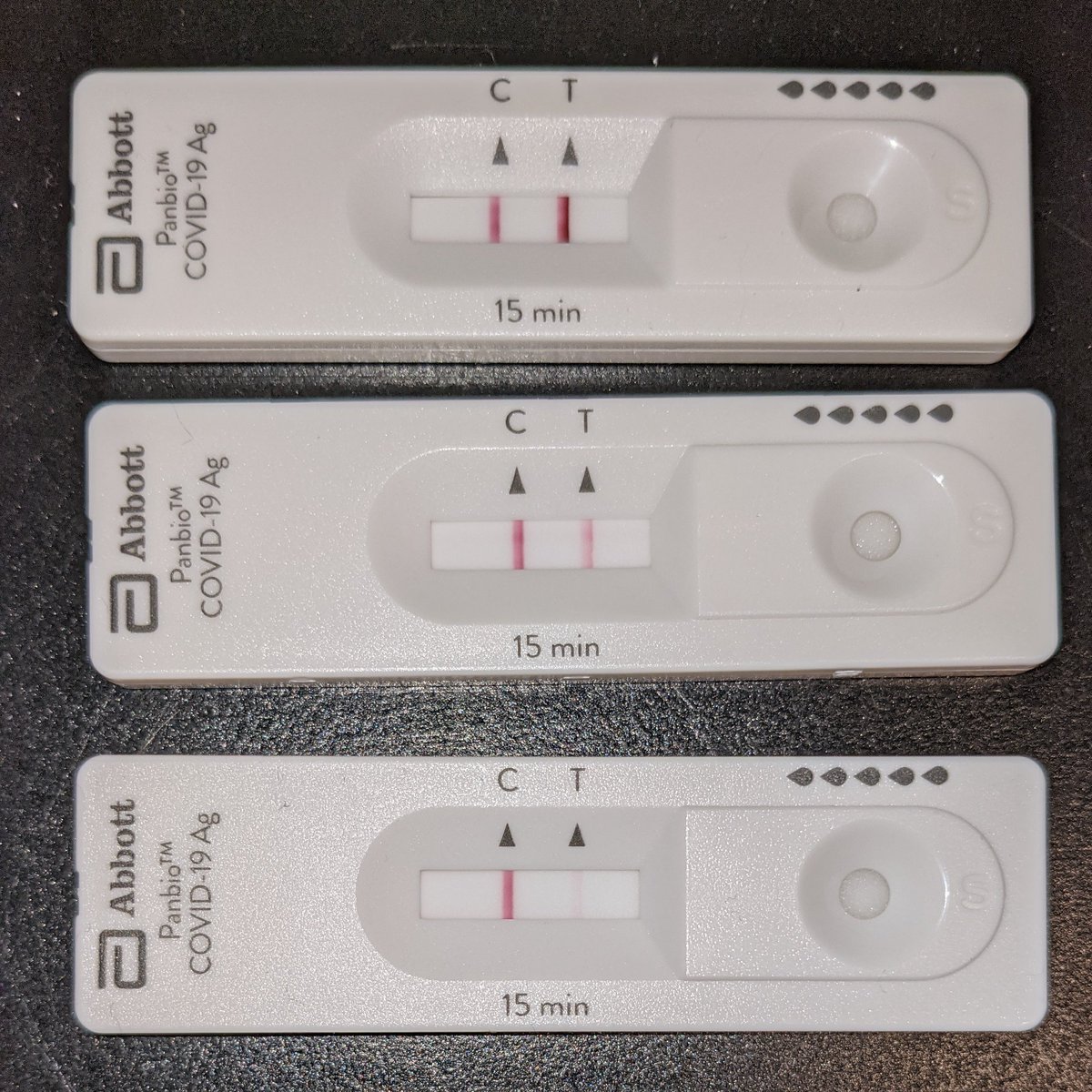
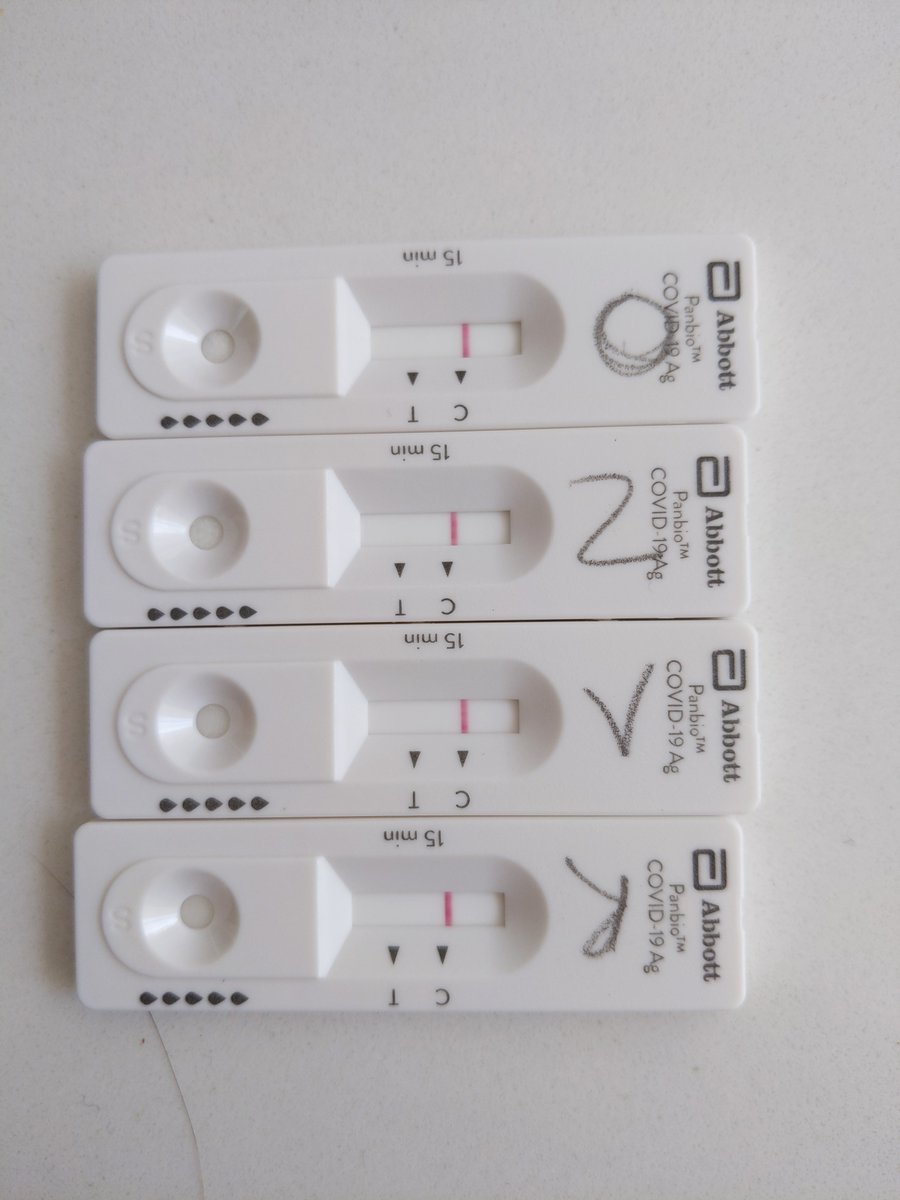
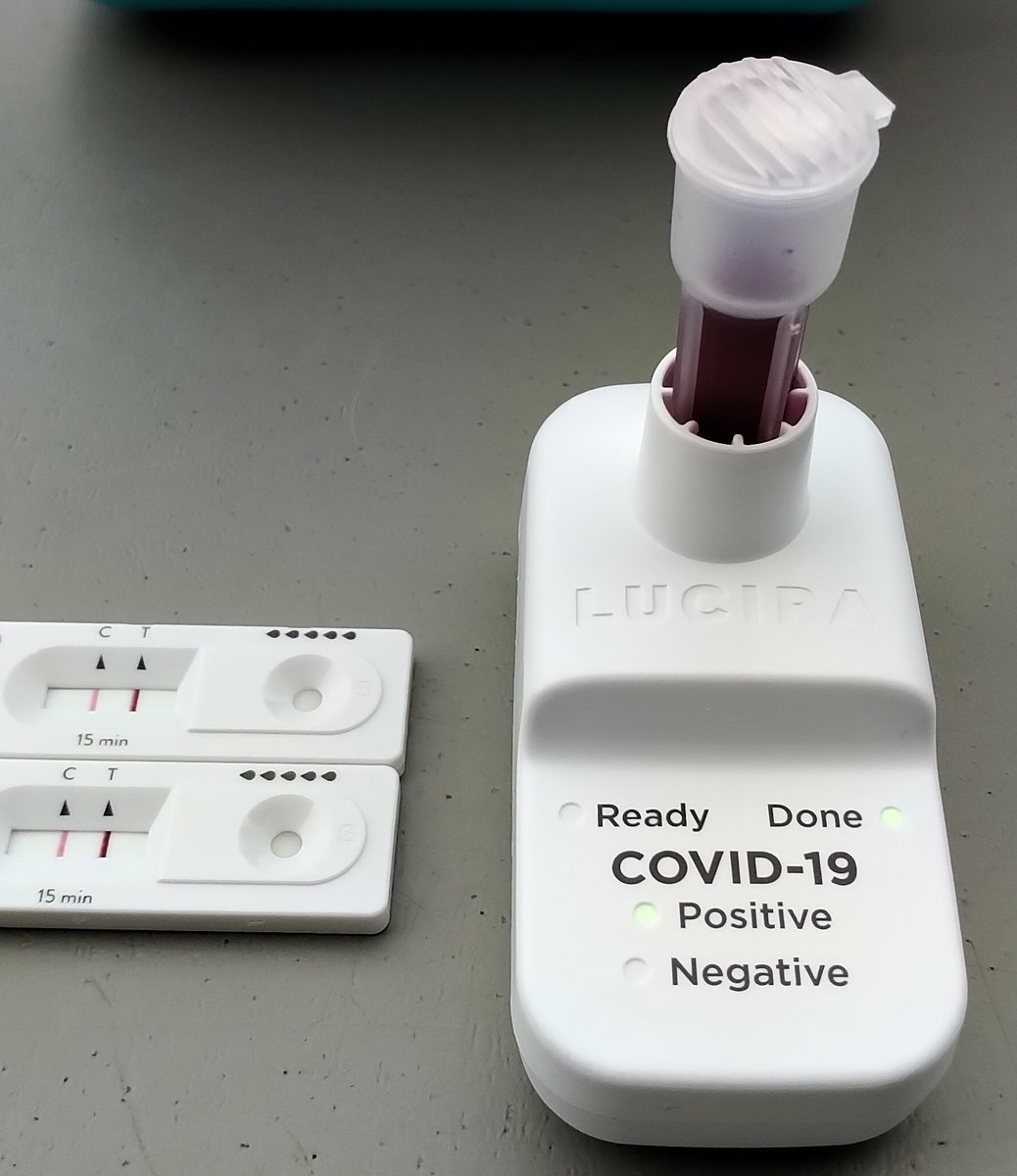
https://nationalpost.com/opinion/np-view-rapid-testings-slow-rollout-just-another-tragic-pandemic-failureTwo positive antigen tests from the #StaySafeScreen bus (one so faint it’s almost invisible here), alongside synthetic positive tests at 1x, 10x and 100x dilutions for reference.
This is what catching sneaky asymptomatic COVID looks like in practice!
It always seemed like quite a coincidence that SARS-CoV-2 was first detected in a city with one of the world’s most active coronavirus research labs. Can it really be an even bigger coincidence that staff were hospitalized in Nov 2019? https://www.reuters.com/business/healthcare-pharmaceuticals/wuhan-lab-staff-sought-hospital-care-before-covid-19-outbreak-disclosed-wsj-2021-05-23/
I’m no conspiracy theorist, just a follower of Occam’s razor.
Imagine, this whole pandemic may be due to one lab tech or field researcher getting sloppy in their use of PPE and accidentally exposing themself to a bat virus!
“Around 60 to 70 percent of the time that you’re PCR positive you are post-infectious. What that means is that the vast majority of people that we detected and isolated, we isolated in error — or rather, people isolated when they probably didn’t have to.” https://x.com/j_g_allen/status/1395188520478781442
I need to update my analogies.
I’ve been saying rapid antigen testing can feel as normal as flossing your teeth. I just realized I’ve done an antigen test 6 times in the past week and only flossed 4 times. It’s starting to feel more like brushing my teeth than flossing them!
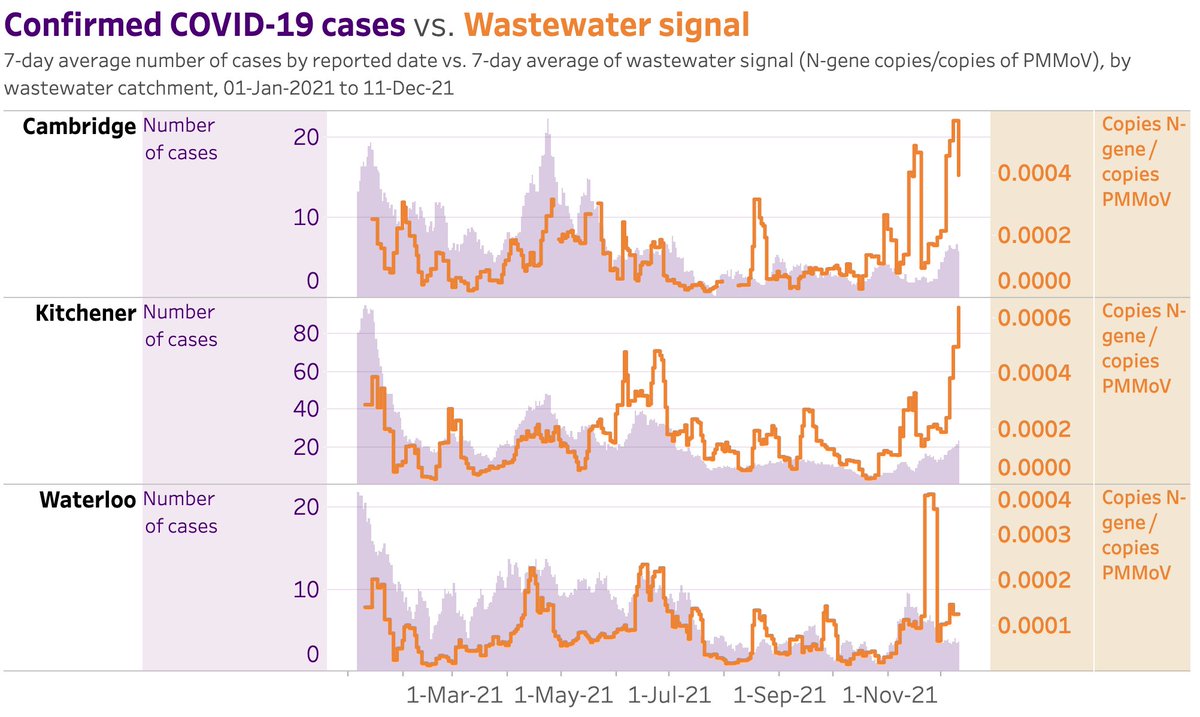
Great to see a wastewater COVID surveillance dashboard online for Waterloo region: https://www.regionofwaterloo.ca/en/health-and-wellness/covid-19-wastewater-surveillance.aspx
As infections move more to the younger unvaccinated population who are also less likely to be symptomatic, this helps indicate how much we’re missing with testing.
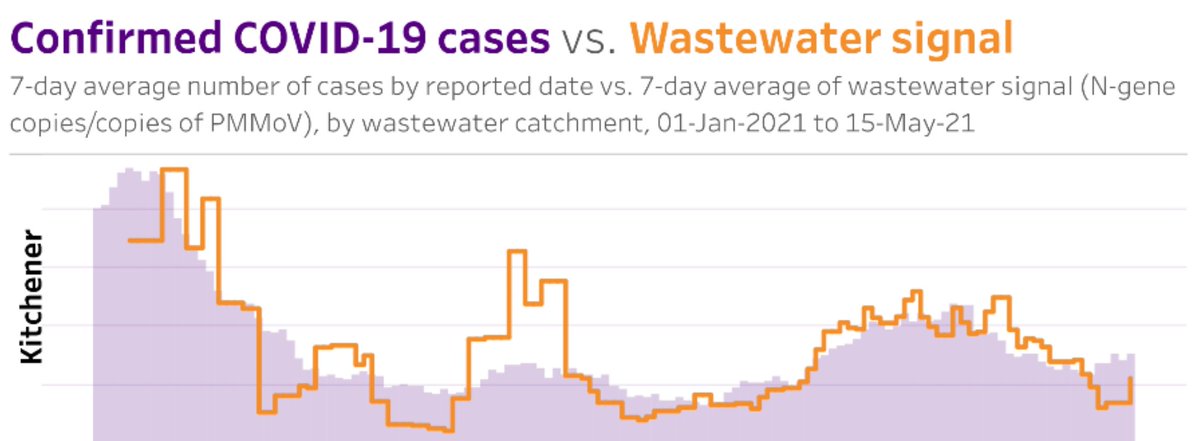
Hopefully regular wastewater surveillance of respiratory pathogens becomes common practice in the future. We have complicated surveillance to help us answer “should I wear a raincoat today”, why not also “should I wear a mask”?
The history of public health is full of frustration getting people to accept new ideas, which in retrospect appear so obvious. Thank you @michaelmina_lab, to my family and other fellow #StaySafeScreen volunteers, you are our John Snow 🙏😁.



For anyone interested to learn more of this history, here are some of my favs:
The Ghost Map: https://g.co/kgs/dVJRnr
Our go-to family car ride podcast: @tpwky
The Premonition: https://g.co/kgs/nZGzBZ
Hey @michaelmina_lab, widescale deployment of antigen testing is still being held back in part due to the real costs of false positives. I’ve heard you say to use rapid nucleic acid for confirmation, but those aren’t always available in all settings (eg. UK home use). 1/
A RAT manufacturer has told me they expect false positives to be random events, generally not correlated with anything in the sample. In practice I’ve seen this - people retest 2 or 3 times and get negative every time (then negative PCR). 2/
So why not just suggest confirmation by 2 or 3 repeated antigen tests, where any one is interpreted to mean a true positive? 3/
Some quick and dirty math suggests this turns a 99.8% specific and 80% sensitive test into a 99.9992% specific and 76% sensitive one. Or, for 3x, a 99.9988% specific and 79.2% sensitive one. 4/4
An antigen test 30 minutes prior to boarding is so much more “sensitive” and specific for current COVID transmission risk than a PCR test 72 hours in the past. https://x.com/DrMCGregoire/status/1404304145818034179
Apparently Twitter believes the FDA logo is “sensitive content”. Either it’s being REALLY smart about what I find objectionable, or really dumb 😂.
@michaelmina_lab, you too?

Hey @ResortsOntario, my family is having a great regenerative time at one of your member resorts this weekend. As someone with an unvaccinated child and concerned with COVID protocols, I feel quite safe. Thank you for your support of a safe reopening of the industry!
That said, I’ve seen unmasked staff talking closely with guests outdoors, and lots of staff mingling closely without masks indoors. With delta having an R0 of 5-8 and full vaccination being a couple months out for many young employees, some staff outbreaks seem sadly inevitable.
If you’d have any interest in helping your members leverage free rapid tests to reduce this risk with a minimum of hassle and cost, I’d be happy to advise. I’m a volunteer strategic advisor for COVID testing at Communitech, working with Health Canada.
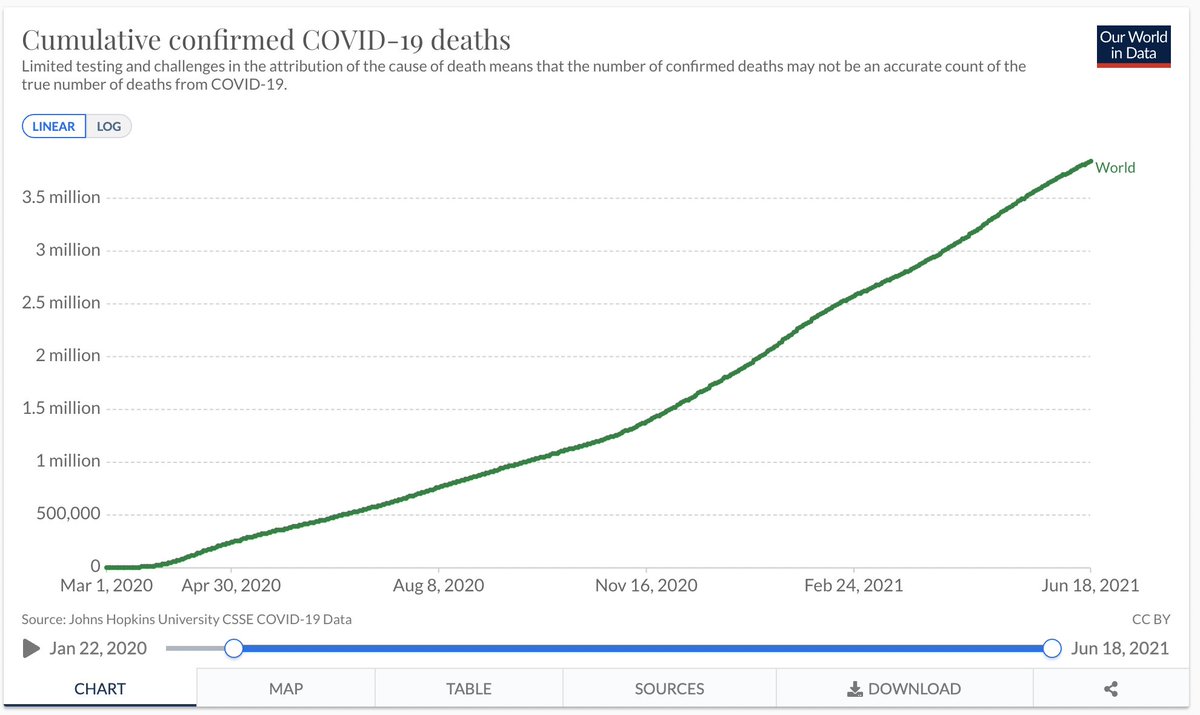
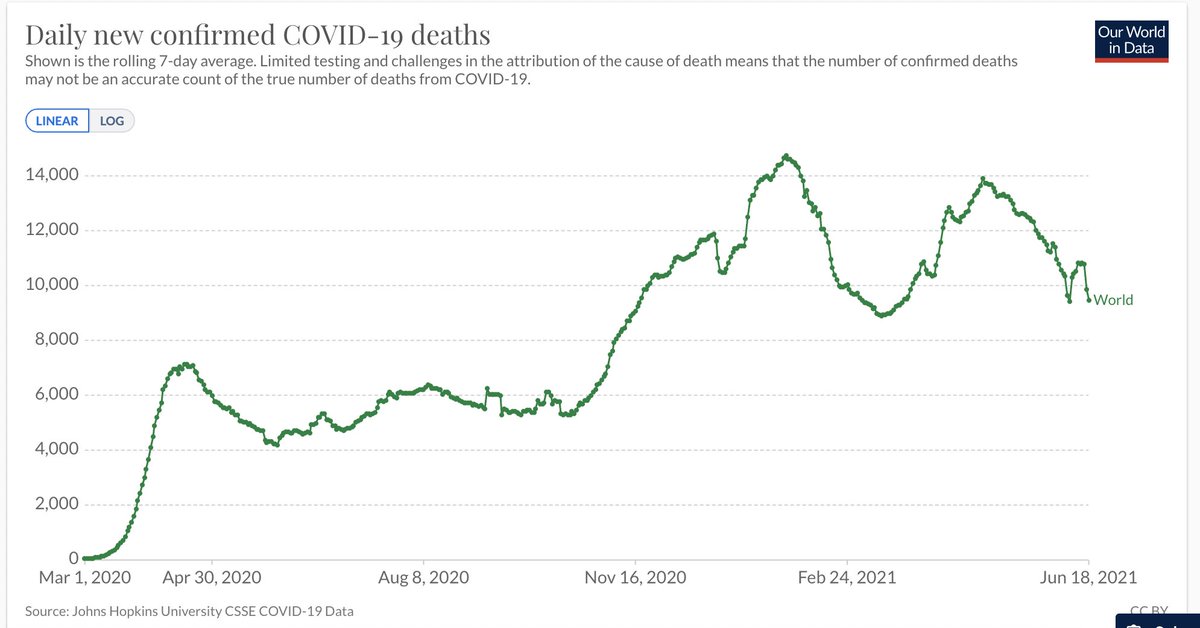
I know we’re all anxious to put this thing behind us, but it seems a wakeup call is in order. Around the world we’re loosing the equivalent of 50 jetliners full of humans every SINGLE day, and its not clearly slowing down yet! History will judge the level of concern we show!
Fascinating. This is a different sort of “genetic archaeology”. Now why on earth would researchers request the deletion of early SARS-CoV-2 sequences from a public database? 🤔 https://x.com/jbloom_lab/status/1407445604029009923
“It’s like you’re in the wrong job there, buddy” 😂 Right on.
If your job is to help guide us with our health and you aren’t willing to be vaccinated, then you aren’t qualified to guide us (rare medical exemptions aside). It’s not “forced”, it’s having the skills for the job. https://x.com/DanielGriffinMD/status/1407652109911302147
It’s as if in software, someone complained about being “forced” to use e-mail because they were baselessly afraid they might get carpal tunnel syndrome despite training. Sorry buddy, your beliefs preclude you from doing your job effectively, please find a different one.
I’m now an AstraZeneca Pfizer hybrid 🎉. Very impressed by the mass vaccination clinic and what that volume of doses will mean for our community in the next months 😁.

Of course, as impressive as the mass clinic was, it’s hard to beat the experience of my first dose: in and out of a small family pharmacy with few other people around.
“No you’re ridiculous! If public health tells you to stay home, you stay home!”. You tell em @BTA_Liz! 😍
https://www.instagram.com/reel/CQhCQXSAGmu/
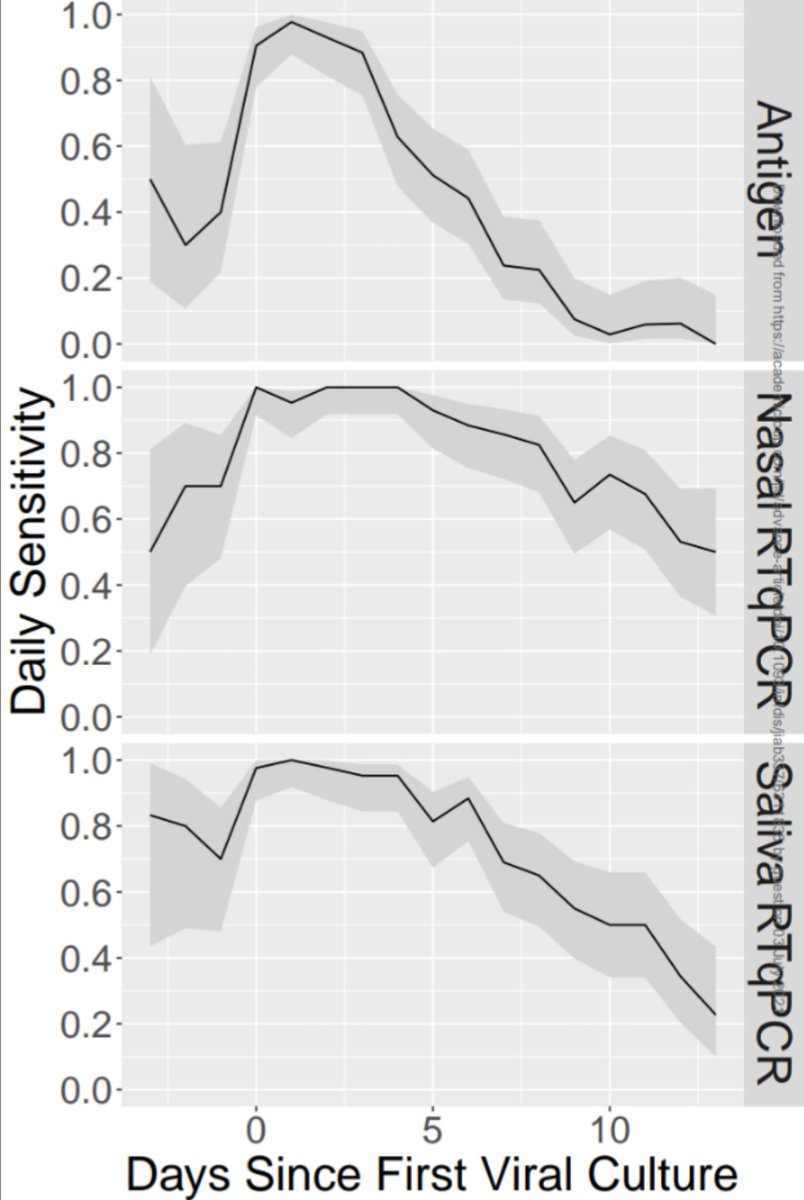
A weekly PCR test has only a 60% chance of identifying COVID while someone is infectious. This rises to 85% when done every 3 days. Daily antigen testing is far more practical than either and achieves 90%. https://x.com/DavidJuncker/status/1411070440836055044
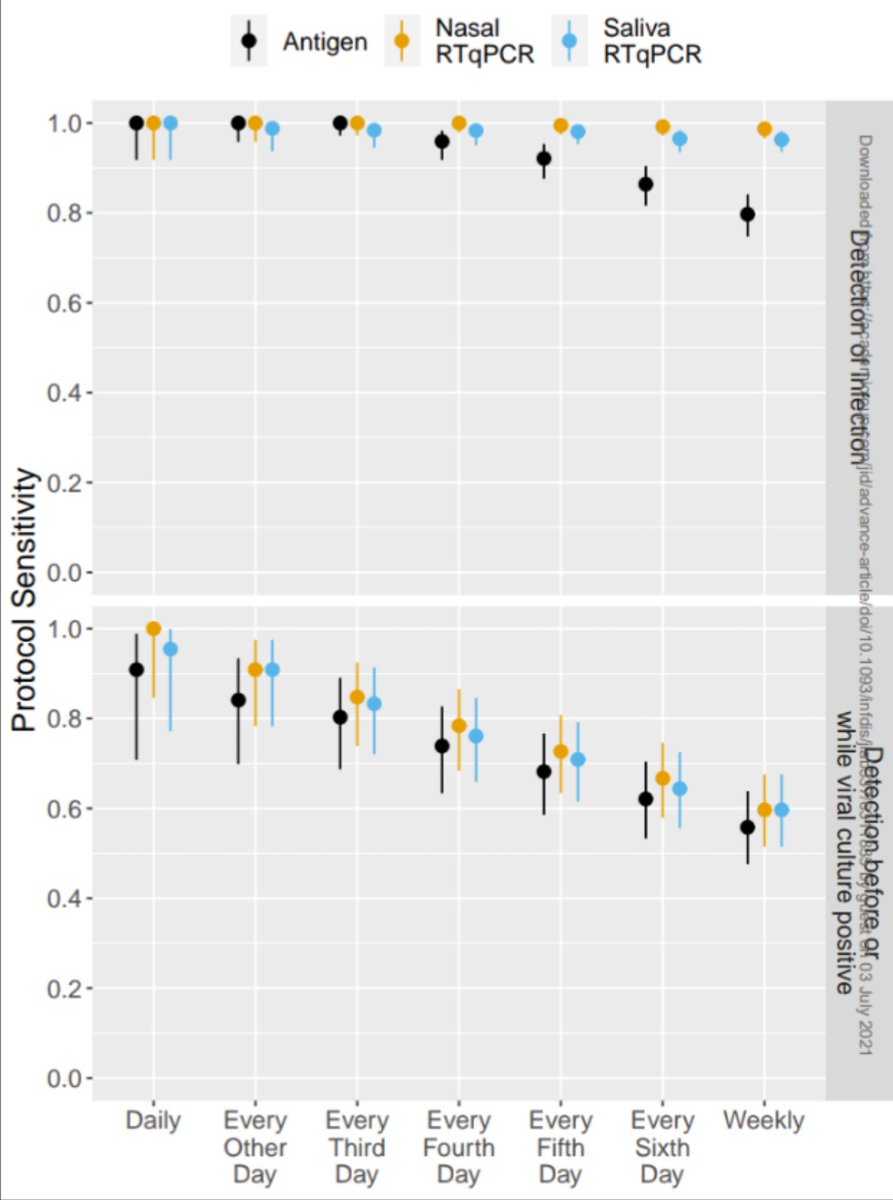
Yes, PCR is better at detecting the virus before contagiousness, but not incredibly so: 70% the day before vs 40% for antigen. Once again, if your goal is to prevent spread, frequency and turnaround time of testing matters MUCH more than analytical sensitivity.
In Waterloo region, one of Ontario’s last COVID hotspots, it’s now possible to sign up to run your own rapid testing pop-up or to be a raid testing community ambassador: https://staysafescreen.ca/
3.4% of Canadian Children had COVID before April. Sure most will be fine, but some will have lifelong effects and others will have contributed to spread reaching vulnerable populations.
Unvaccinated kids using rapid tests in the fall could be key to avoiding another surge. https://x.com/DGBassani/status/1412546197231968256
For the first time in about 9 months, Ontario reported zero COVID deaths yesterday!
https://covid-19.ontario.ca/data
Rather than all the “we’ll have to live with COVID like we live with Flu” talk, I’m excited for the reverse: Let’s crush Flu (and RSV, and all Coronaviruses) with vaccines like we’re learning to crush COVID!
We’ve been so complacent in assuming that colds are a fact of life. https://x.com/DanielGriffinMD/status/1413210011065520128
Bravo! All health workers (and high school students) in the UK have been doing home testing for months, why is this so controversial? You can’t go to a bar or restaurant in Germany without proving you’re fully vaccinated or have a negative rapid test that day. Get with it Canada! https://x.com/bradwouters/status/1412781484151279616
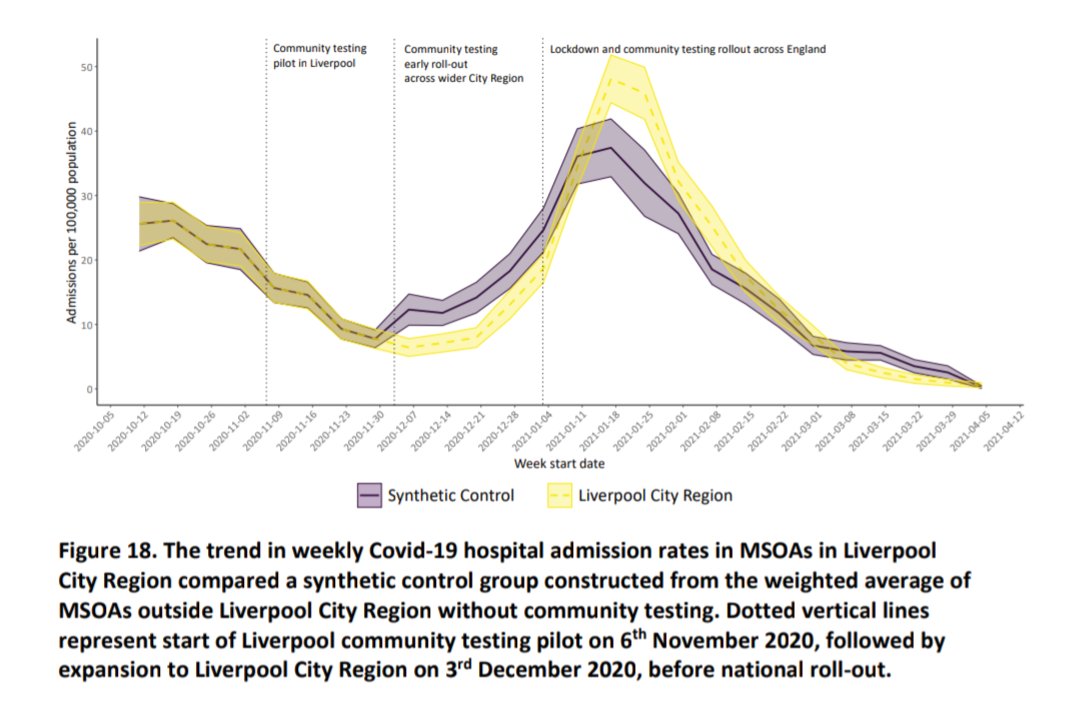
Once again, it’s clear that when rapid tests are deployed at scale, cases fall faster.
”It is estimated that Liverpool’s community testing led to an 18% increase in case detection and a 21% reduction in cases compared with other areas”
https://news.liverpool.ac.uk/2021/07/07/liverpool-covid-19-testing-pilot-cut-virus-cases-and-spread/
“these tests are effective when used regularly, with only a small change in effectiveness between experienced test users like professional laboratory scientists or nurses and inexperienced test users.” https://www.gov.uk/government/news/asymptomatic-testing-backed-by-new-research-studies
Also home-use rapid tests FTW: “Galbraith’s friend had access to a number of antigen tests at home so she decided to test Julian, just in case.” #StaySafeAmbassador https://x.com/FourWinns298/status/1414735956024954880
Even the best experts are misled by reading only the abstract 😉.
Abstract claims “100.0% sensitivity and specificity”. Have to hunt through the body to find n=10, with only 3 positives 😂. The extra “.0” in particular is a rediculous lie. https://x.com/RickByersLab/status/1414797041373519873
I got vaccinated because I consider it an ethical responsibility to society to ensure I don’t contribute to the spread of a disease that has already caused 4 million deaths and immeasurable suffering. #WhatsYourWhyWR
Sadly this should be a surprise to exactly nobody who is paying attention. At current vaccination rates, it’s gonna get a lot worse in many US states before it gets better😢. https://www.cbc.ca/news/world/us-covid-rising-rates-1.6101365
And please let’s not forget - fully 1 in 500 people (0.2%) in the US have died of COVID already, for a disease that’s was predicted to have an infection fatality rate of <0.5%.
Predictably, outbreaks are starting at kids camps. My family is volunteering to run free rapid self-testing for campers, but so far no camp organizers are interested. https://kitchener.ctvnews.ca/waterloo-region-reporting-covid-19-outbreaks-at-two-day-camps-1.5512730
This is pretty worrying. It means we likely won’t get herd immunity protection afterall and we should probably plan for everyone to be infected. No big deal for many, especially the vaccinated, but still deadly for ~0.5% of the unvaccinated adults. https://x.com/DanielGriffinMD/status/1416811168614735872
The OST report on schools argues against serial rapid testing (https://covid19-sciencetable.ca/sciencebrief/school-operation-for-the-2021-2022-academic-year-in-the-context-of-the-covid-19-pandemic/#:~:text=Asymptomatic%20screen%20testing%20(i.e.%2C%20asymptomatic%20testing%20in%20the%20absence%20of%20documented%20exposure)%2C%20is%20not%20routinely%20recommended%2C%20especially%20in%20the%20low%20to%20moderate%20COVID-19%20risk%20scenarios.). It cites one short letter which claims antigen testing is “low-yield”: https://www.cambridge.org/core/journals/infection-control-and-hospital-epidemiology/article/low-yield-of-severe-acute-respiratory-coronavirus-virus-2-sarscov2-asymptomatic-routine-screen-testing-despite-high-community-incidence/176BA478C1D529E0DACCE0D6FA8DADC0
This conclusion comes from serial antigen screening having a positivity rate of “only” 0.36% at a time when the weekly case rate in Ontario was 0.1% and public health test positivity rate was 5%. Comparing positivity rates like this is flawed logic.
If you take the high risk people out of the pool (symptomatic / close-contact) then of course those remaining will have a lower risk of being infected. But rapid testing STILL caught cases at 3x the presumed prevalence, suggesting public health containment was completely failing!
The important comparison is not positivity rates but cost of interrupting one transmission chain. If you give antigen tests to people to do at home and have rapid molecular testing handy to confirm any positives, they can be about 1/10th the cost of PCR tests.
The question is: how much value is there to society in each COVID transmission that gets interrupted (that case and all downstream cases)? I don’t know how to calculate that, but in the cited study, if done efficiently it would have cost about $2000.
I don’t know how the authors of this paper would compute a value for human suffering, but calling $2,000 (or even $20k, assuming 10x admin overhead) to prevent a nursing home outbreak “low yield” and “not cost effective” seems pretty callous and inhumane to me.🤷
The OST report on schools expresses concerns over equity of access to rapid COVID tests (https://covid19-sciencetable.ca/sciencebrief/school-operation-for-the-2021-2022-academic-year-in-the-context-of-the-covid-19-pandemic/#:~:text=There%20are%20substantial%20logistical%20and%20equity%20concerns%20that%20need%20to%20be%20taken%20into%20consideration). I agree with this concern. 1/
The situation today is that pro sports players, many politicians, employees of Canada’s biggest companies (Air Canada, Rogers, etc.) and rich white dudes with the educational privilege like me are all keep our families safe by regular rapid testing.
With our #StaySafeAmbassador program (https://staysafescreen.ca) we’re giving free access to anyone willing to help spread the word in the Waterloo region. But that’s not nearly enough.
My daughter’s private school makes regular use of rapid COVID tests. I took her out of public school due to very poor COVID protocols.
How on earth can keeping these tests out of public schools possibly be an equity “improvement”?
Why is there so much concern over the 1 in 500 risk of false positive with antigen tests but nobody is asking “what’s the false positive rate of COVID symptom screens”? Surely having an unusual headache, stuffy nose, cough or fever that isn’t COVID is more common than 1 in 500!
I’m proud to work for a company which requires proof of COVID vaccination (or medical exception) to come into the office, and also is enabling a significant chunk of our workforce to continue to work from wherever they feel most productive. https://blog.google/inside-google/company-announcements/vaccines-and-our-return-to-office-plans/
More evidence that our vaccines do not provide much sterilizing immunity against delta 😥:
An outbreak in the US with 469 cases, 90% delta, 74% fully vaccinated. Population vaccination rate 69%.
https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm
“[Delta] means that we are going to want to place more weight on rapid antigen screening both in the workplaces, schools and other areas and also for at-home testing.” https://x.com/joshgans/status/1421187699793408001
We weren’t sure we’d get sterilizing immunity, then we did, now it looks like we’re losing it. The important response is not “this is what we always said”, it’s “crap, what can we do NOW to get this awesome protection back?”
To be clear, yes of course the MOST important role of the vaccine is to prevent serious disease (and yay, we still have that). But preventing serious disease in those who can’t or won’t get vaccinated was a pretty damn valuable property too.
“I’d rather have questions that can’t be answered than answers that can’t be questioned”.
What a great, and relevant, quote from Richard Feynman, via the awesome @DanielGriffinMD. https://x.com/profvrr/status/1421443197562146819
Today in Canada, having the peace of mind and extra safety of having rapid COVID tests at home is mostly a privilege of the rich. We’re trying to change that! #StaySafeAmbassador https://www.therecord.com/news/waterloo-region/2021/08/05/rapid-covid-19-testing-influencers-needed.html
“While Delta means that permanent herd immunity has become even more elusive—perhaps impossible—a state of temporary and reliable herd safety can be achieved tomorrow.” https://insidemedicine.bulletin.com/378975113857960
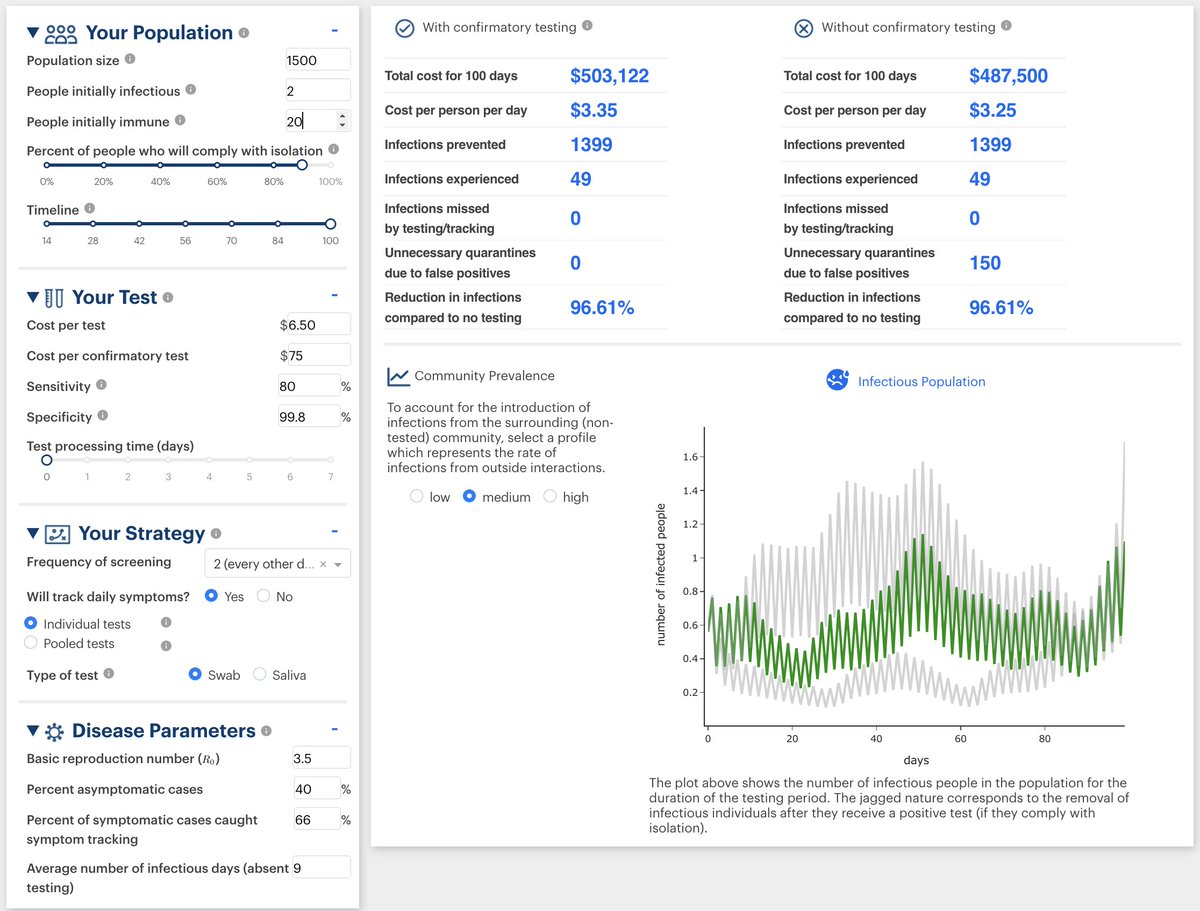
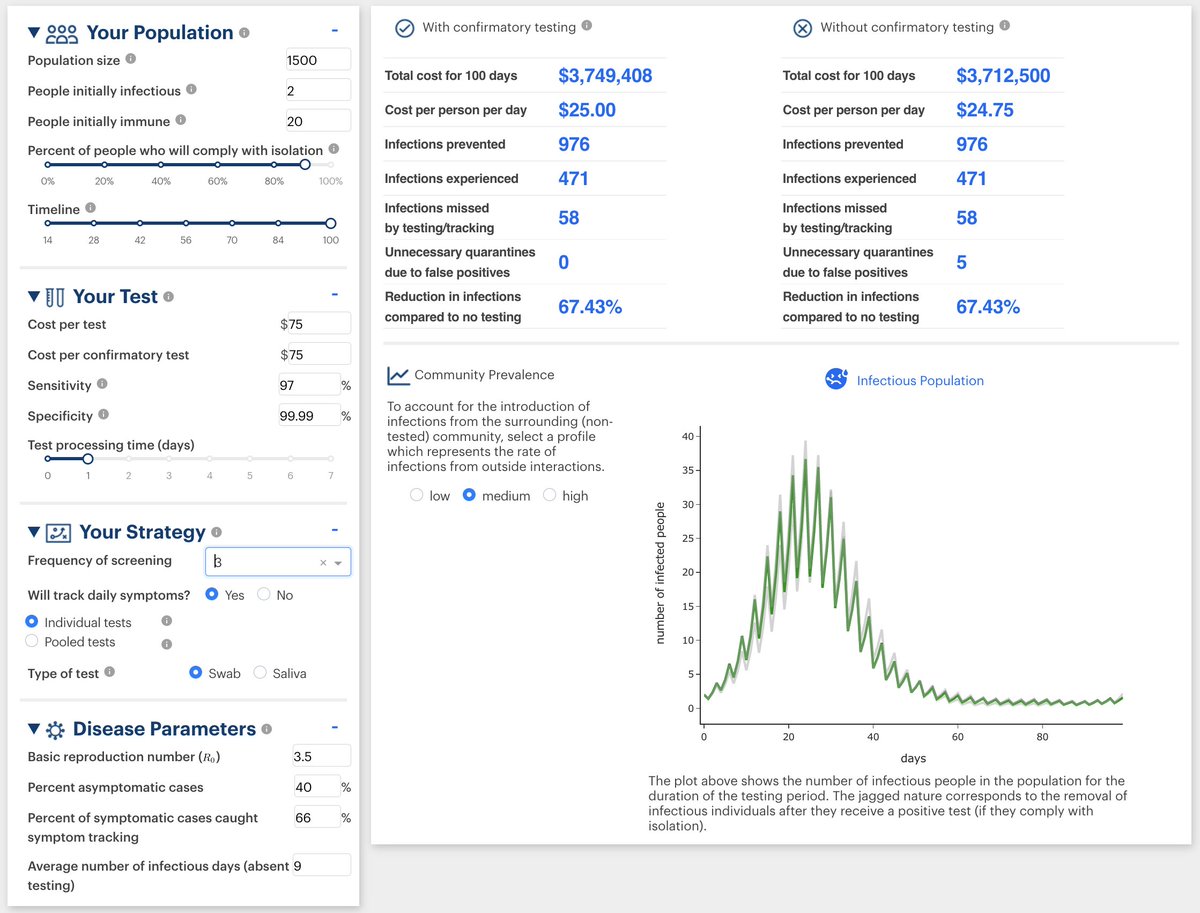
Wow, what a great tool!
https://calculator.unitedinresearch.com/simple_dashboard
Needs update for larger R0 for delta, but still very useful. Comparing alternate day Panbio (first) to lab PCR testing every 3 days (second). Why are we still debating this? https://x.com/DanielGriffinMD/status/1424939610870796295
Hey 🇨🇦Canada🇨🇦, we could effectively end this pandemic now by:
➡️ Making rapid tests available to everyone for free (~$1B/month)
➡️ Requiring a rapid test within 48 hours to enter any building outside your home
Is the alternative of a 4th wave really the choice you prefer?
Some experts have been saying this for a year: https://time.com/5912705/covid-19-stop-spread-christmas/. The evidence and understanding keeps getting slowly stronger. Where is the tipping point?
This isn’t “expensive”, it’s the bargain of a lifetime compared to the alternative!
And since this apparently still needs to be said explicitly: of course we also need everyone to be vaccinated! But no, sadly, it doesn’t look anymore like that will end the pandemic on its own, at least not without boosters for all. 😥 https://www.cdc.gov/coronavirus/2019-ncov/variants/delta-variant.html
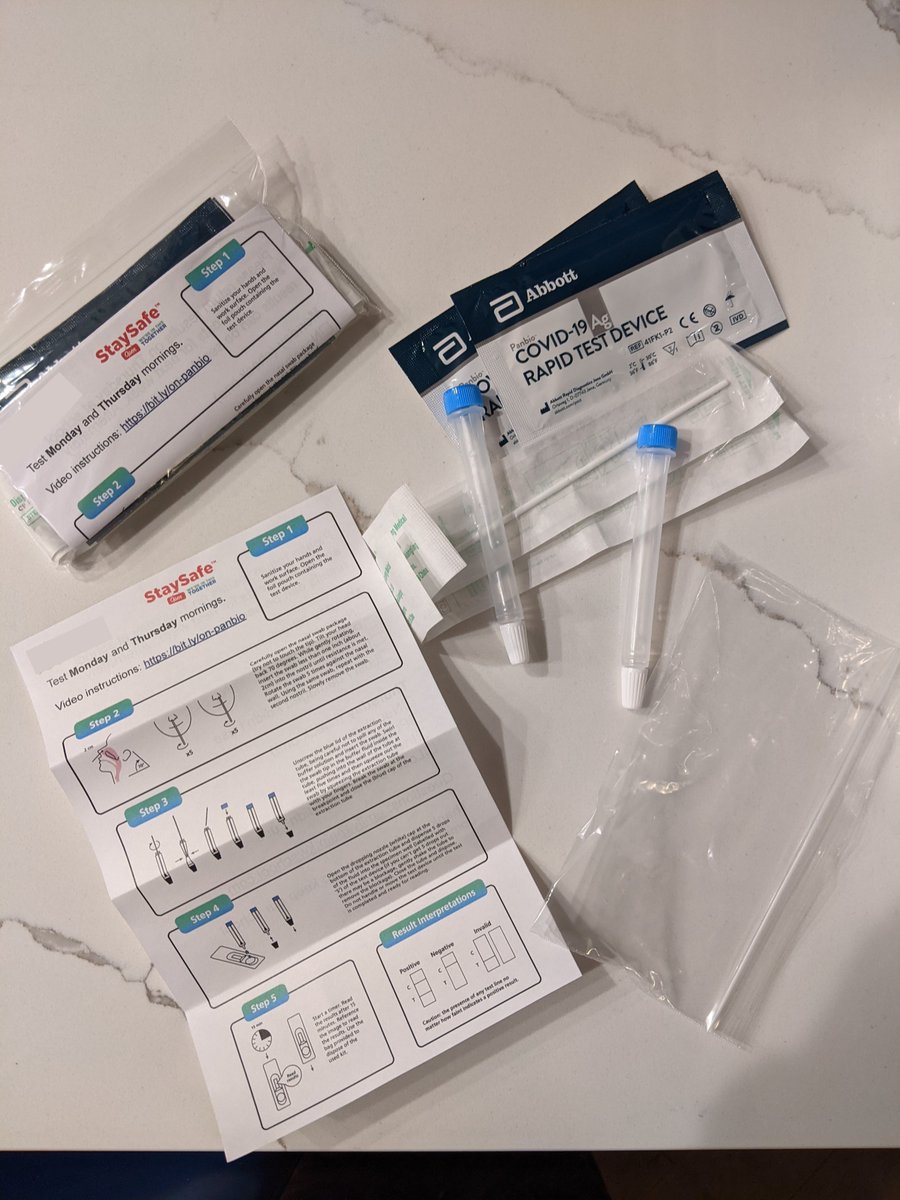
In the https://staysafescreen.ca/ community testing program we’ve been using a new type of screening test with amazing properties:
78% sensitivity
99.996% specificity
<$7/test (90% gov’t subsidized)
Avg. 15 minutes for negative, 45 min for positive
Best of all: already HC approved!
It’s simply an Abbott Panbio antigen test, with presumptive positives followed up with a Lucira check-it rapid molecular test.
Fast, cheap and sensitive enough to be a highly effective screening tool but with almost zero false positives.
And in case it’s not clear, this is still just a “screening test”, not a medical diagnostic. We always encourage presumptive positives (even with a positive rapid molecular test) to go to public health for confirmatory PCR testing.
👎Bad news: waning immunity 6 months after getting vaxxed is likely a big deal.
👍Good news: dosing intervals around 8 weeks likely offer more durable protections (yay Canada!)
∴ It’s time to plan boosters for all! https://t.co/qwSZjNb22R
Great quick interview with @EricTopol:
➡️ Waning immunity is a real issue with delta
➡️ Germany doing so much better than the US perhaps due to widespread use of rapid testing https://x.com/MedCramVideos/status/1425657484102959104
Breakthrough infections appear just as contagious as for unvaccinated infections. But I don’t think we should be resigned to all get it just yet! We need delta-formulated boosters, and to suppress spread with mandatory rapid testing until then. https://x.com/DanielGriffinMD/status/1426021672222699523
Today’s biohackers are the garage computer hackers of the 70’s.
What’s the equivalent of the smartphone which our grandkids will take for granted 30 years from now? https://x.com/roamfu/status/1427270426212724740
I really hope someone is studying waning immunity in Canada, looking also at dosing interval. https://x.com/segal_eran/status/1427696623988117505
@uhwuhna, I’ve personally observed many folks in the liberal Health Canada administration bend over backwards trying to give away rapid tests and expand access. Obviously I wish they could/would do more still. This report sums it up: https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/medical-devices/testing-outreach-collaboration/industry-advisory-roundtable/reports/taking-stock-looking-forward.html
[Replies were locked] https://x.com/uhwuhna/status/1428814495053451269
The hospitalization risk of the vaccinated is a key trend to watch. It, more than anything else I think, will predict how and when this pandemic ends. Will it hold in Canada (perhaps due to our extended dosing) or rise significantly 6+ months post vaccination like in Israel? https://t.co/mh7qkT6pL8
Yikes. @DFisman was the one person on the OST who I felt I could understand and trust. Are there others active on Twitter I should also follow to get a contrary but honest perspective? https://x.com/DFisman/status/1429761663671185413
To what extent are monoclonals being used in Canada? https://x.com/DanielGriffinMD/status/1429776444234862598
Just listened to an excellent account of the history of hand washing in obstetrics by @tpwky: https://thispodcastwillkillyou.com/2021/05/18/episode-73-puerperal-fever-seriously-wash-your-hands/.
Why did it take decades after compelling evidence existed for doctors to accept that washing their hands would save lives? Is this problem entirely solved now?
If we can make rapid testing an easy part of everyday normal life (like brushing your teeth) then we may never need to lockdown to contain a pandemic again!
Sadly, the direction we’re headed in Ontario I think means that by the end of the year we’ll either be dependant on heavy lockdowns again or there will be a lot of suffering. Vaccines mandates are great, but insufficient on their own now. 😢
15 months ago I predicted the cost for PCR machines would fall quickly from the $13,000 I spent on mine to affordable for home use. But I totally failed to predict we’d have single-use disposable molecular tests in little more than a year! https://x.com/RickByersLab/status/1393219385469325313
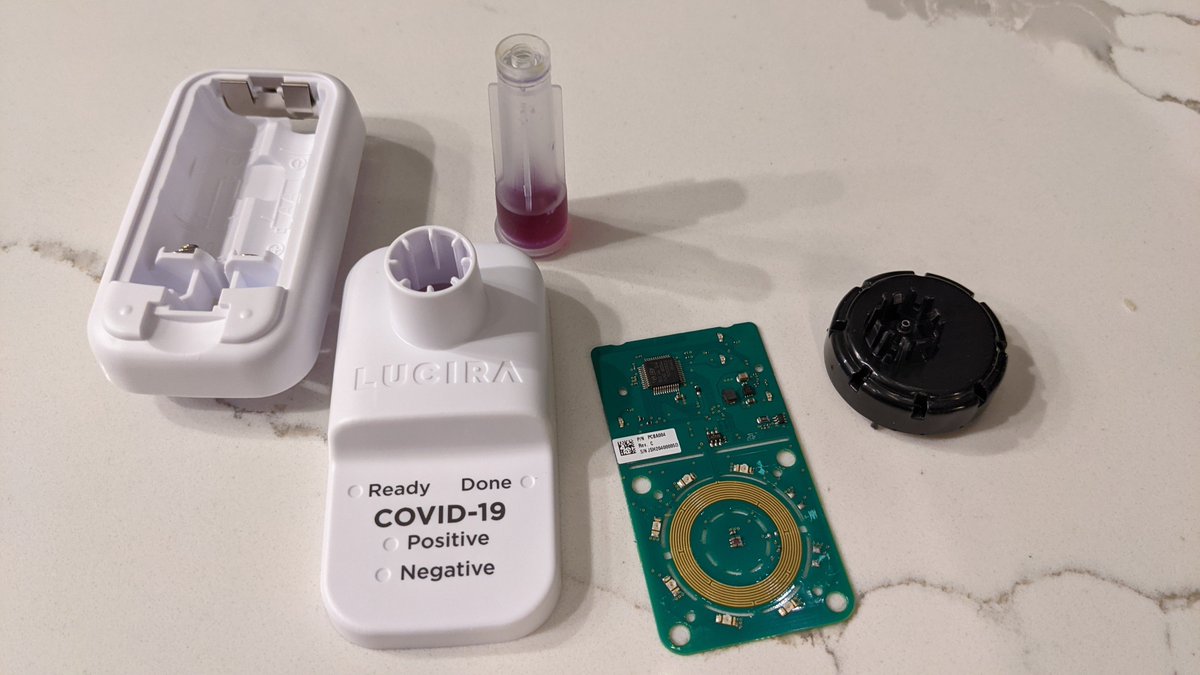

This is a Check-It (https://www.lucirahealth.com/) RT-LAMP device. Looks like 8 wells (only 6 illuminated), 2 positive controls and a CCD sensor for taking a photo of the colorimetric reaction. Seems so wasteful to be disposable but super cool!
The data are clear, this fall we MUST reduce the opportunities the virus has to spread. Lockdowns work by reducing contact between everyone, rapid tests work by reducing contact specifically for those most likely to be contagiousness. The choice is ours. https://x.com/BeateSander/status/1433477655505129473
Winter is Coming to Ontario.
“There’s no shame in fear, my father told me, what matters is how we face it."
"Sometimes there Is no happy choice, only one less grievous than the others.” https://x.com/BeateSander/status/1433477672827555849

But there’s another John Snow I respect more. He would tell us to ruthlessly hunt down the path of transmission, and put a stop to it - even when many of the experts think you’re a fool. https://en.wikipedia.org/wiki/John_Snow


Rapid tests do a damn good job showing where COVID transmission is likely to come from. Let’s require their use broadly to avoid the need for another lockdown and further avoidable suffering.
@michaelmina_lab @TestandTraceCa @cdlscreening @LisaBarrettID @DFisman
The argument that medical masks and respirators need to be preserved for healthcare is horribly out of date.
If you want to support healthcare workers, buy and use medical masks. It props up manufacturing capacity and lowers transmission. https://x.com/BarryHunt008/status/1434008754060660738
@UWaterloo is making free at-home rapid COVID tests available to all students and staff: https://uwaterloo.ca/coronavirus/testing-rapid-screening-and-vaccinations#screening. Great leadership! This should be extended to every school at every level across Canada.
I’m working with a few Canadian public school parent groups and private school administrators to get them free rapid COVID tests for kids to voluntarily use at home before school. If you’d like to participate, please fill in this form: https://docs.google.com/forms/d/e/1FAIpQLSeyH32XeG2CZJN89pRr7sUr0vzDzrv-8weeYzLqTt17EdpOjA/viewform
For those asking - these are the same Panbio test kits being used in the various Canadian government workplace testing programs. Eg. see Ontario instructions here: https://www.ontariohealth.ca/COVID-19/Health-System-Response-Resources#testing-and-assessment-centres and in particular this video: https://www.youtube.com/watch?v=XP3aqwO5rJo
Correction: despite unclear wording on the page, I have it on good authority that the tests are only provided to people who are unvaccinated. That’s a shame - vaccinated people can still get infected and transmit (but at perhaps 1/8th the rate in Ontario right now).
“We’ve long accepted colds and flus as inevitable facts of life, but are they?”
Waterborne diseases were a fact of life until the sanitation revolution 150 years ago. https://x.com/jljcolorado/status/1435454183746859013
Great coverage of the #StaySafeAmbassador program on CTV News: https://www.ctvnews.ca/mobile/health/coronavirus/experts-recommend-using-more-rapid-tests-so-why-is-canada-so-far-behind-other-regions-1.5578229
“I salute all hardworking journalists who put science and facts at the heart of what they do, and ask me tough questions every day, but make sure they’re educating and informing Canadians from a broad range of perspectives”.
Now THAT’S how a real leader addresses “fake news”! https://x.com/Ben_Parsons__/status/1435799898071310337
Tonight my family put together a bunch of 2-test rapid testing kits for my Daughter’s school to hand out to participating kids tomorrow!
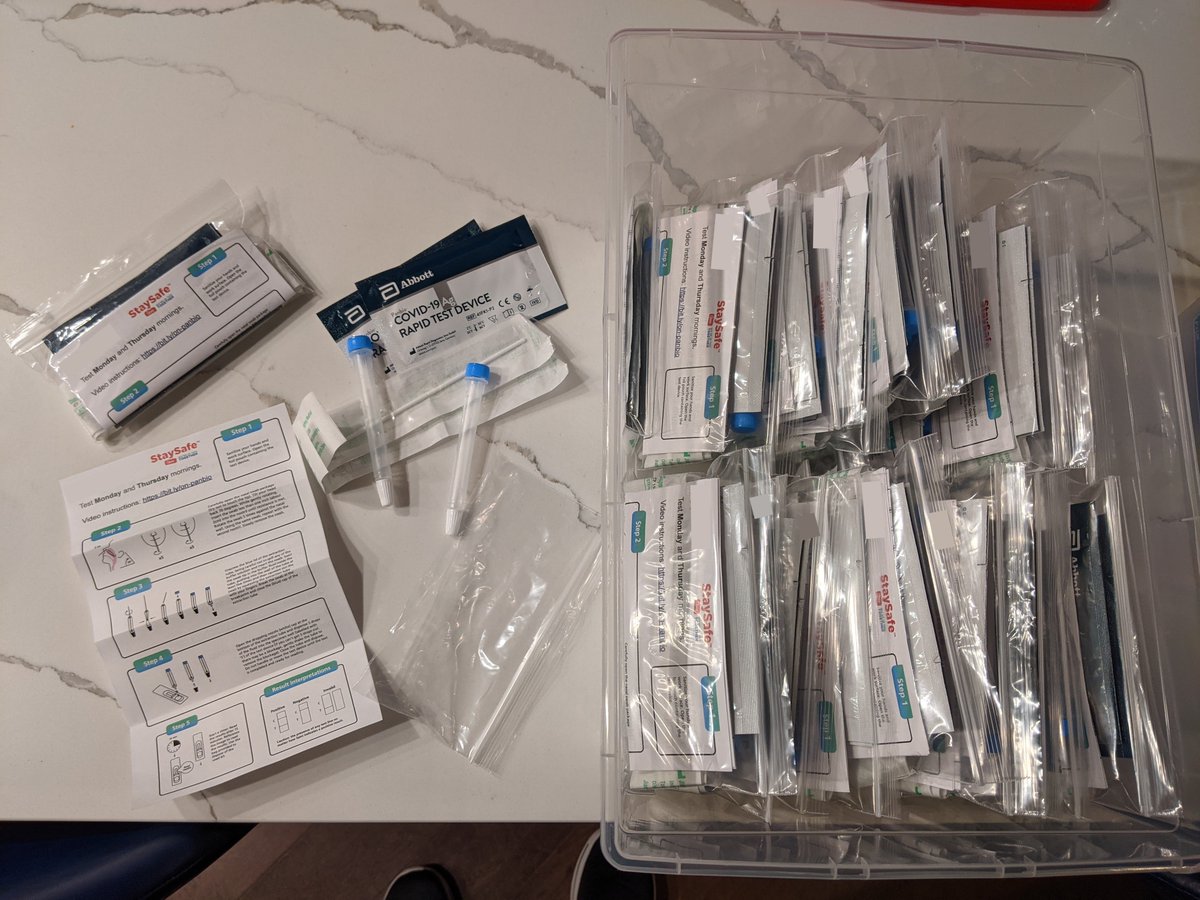
6 days of public school parent group advocacy (no help from the school) and already 1/3rd of the kids in the school have opted into twice weekly home antigen testing. This is phenomenal! Incredible job making your kids school safer @uhwuhna! https://x.com/uhwuhna/status/1436663237538422784
If we decide the 4th wave must be suppressed in Ontario, what’s cheaper - another lockdown or giving every Ontarian rapid tests to do at home every other day?
According to this story, the tests might be about 10% the cost of a lockdown: https://nationalpost.com/news/what-16-months-of-covid-lockdowns-have-cost-us
✋I thought COVID would be about as bad as Flu and that we’d have to all accept just getting it. https://x.com/DrNeilStone/status/1442119888160673800
Hey @DFisman, if rapid tests were in limited supply, how would you prioritize distributing them for maximum society benefit? I’m assuming it takes at least a month to spin up in any given group (education, logistics, etc.).
I’m luck to have had the resources to buy rapid tests for my family since the start of this pandemic (first at-home PCR, then antigen). I have been working to increase equity by helping to lead community programs. Today Dr. Moore shut that down. But I can still donate to this! https://x.com/C19TestFinders/status/1443373826369261568
I know so many people who get rapid tests to take home through their workplace and ultimately use on their unvaccinated kids, but so many others (including teachers) whose employers won’t opt into the program for them. This is a massive equity issue. https://www.therecord.com/news/waterloo-region/2021/10/01/employers-can-get-free-rapid-tests-why-cant-families-get-the-same.html
Best reporting on this issue yet. Great quotes from @AmyGreerKalisz, contrasting Ontario with NS who just starting giving parents tests.
https://www.theglobeandmail.com/canada/article-ontario-tells-agencies-covid-19-rapid-tests-are-only-for-workplaces/4.5M deaths worldwide and counting. All of which could have been avoided with better preparedness and infectious disease control. This is NOT OK. We can and must do better. https://x.com/AmyGreerKalisz/status/1444389262032613376
“This is democracy in action. When the state cannot provide the needed assets, people step up and get it done… they’ll come around eventually like they did with mask wearing” @deonandan Right on!
https://www.cbc.ca/listen/live-radio/1-14-day-6/clip/15869848-episode-566-rapid-covid-19-tests-cindy-blackstock-cystic
“All we needed was access. We didn’t really ask for permission for the rest of it… If you’ve got the kits you can take the initiative. Right now it’s time to beg forgiveness later I think” @LisaBarrettID
#StaySafeAmbassador
https://youtu.be/3rB5SzCgn4A?t=605
This study tells us what to expect from COVID in Canada this winter: lots of infections but relatively low hospitalization rate. But 10% of a big number is still a big number 😥. Hopefully longer dosing interval, boosters and rapid tests will save us from a terrible winter. https://x.com/VincentRK/status/1445164155712032770
Its also interesting to see that all the noise about delta evading vaccine immunity a couple months back indeed seems overblown - minor compared to the effect of waning immunity for all variants.
A few things of note from today’s announcement: https://www.youtube.com/watch?v=j57qp1Ni3DM
Kudos to Dr. Moore for changing his strongly held opinion based on new data around Delta (or at least “newish” from the past few months)
1/
The mention of “at home” testing is absolutely key. This isn’t about healthcare workers / teachers having new responsibilities in classrooms or about take-home swabs that have to be sent to labs, it’s about distributing tools to parents. That’s key for real scale and impact.👍 2/
Empowering local medical officers is also great news IMHO. It means we’ll see some diversity of approach that will enable us to learn and build consensus rather than everyone following the same dictated opinion. Tradeoffs are hard. Experimentation is key. 3/
Lots of emphasis on the true solution being vaccination. This confirms signals I’d been getting elsewhere - that some hesitation to embracing testing was due to the crowd looking for an alternative to vaccination. Lets all be clear: tests aren’t an alternative to vaccination. 4/
Lots of emphasis on being “targeted”. This makes sense when there is supply constraints, which is certainly the case. I am optimistic that strictness of targeting will diminish as comfort grows and supply increases. But this is probably the greatest risk to maximizing impact. 5/
All in all, I think there’s a lot more to do to get rapid tests used at the level that’s likely the sweet spot of Canada-wide cost/benefit tradeoff. But this seems likely to become a very good step in the right direction for Ontario. 6/6
TIL Walmart is doing rapid COVID tests for half the price of Shoppers ($20 vs. $40): https://www.walmart.ca/cp/shop/asymptomatic-covid-testing/6000203002155
That’s a good step in the right direction. A few more price-halvings and we’ll be in the ballpark for real impact 😁
@co2detective, you don’t know what you’re talking about. Rapid tests were never allocated by health unit. Do you really think StaySafe would have been able to give out >400,000 tests if tests were proportioned equally by health unit?
Exactly! Even a “low” 40% positive-predictive-value is a hugely valuable way to use our limited PCR resources and keep total isolation to a minimum. https://x.com/McDevonMD/status/1445876759556096001
While antigen false positives are certainly an issue, this article highlights that false negative PCR results definitely also occur. We need to stop thinking of a single negative PCR test as some sort of gold standard diagnosis.
+Antigen & -PCR isn’t always a false positive! https://x.com/Kit_Yates_Maths/status/1446025535147098117
I’ve just had the first cold go through my house since I built my home microbiology lab. qPCR test results are in and it’s definitely Rhinovirus (green line at cycle 25, earlier green line is external control “B2M”). This is a big day for my long-time dream of home virus testing!
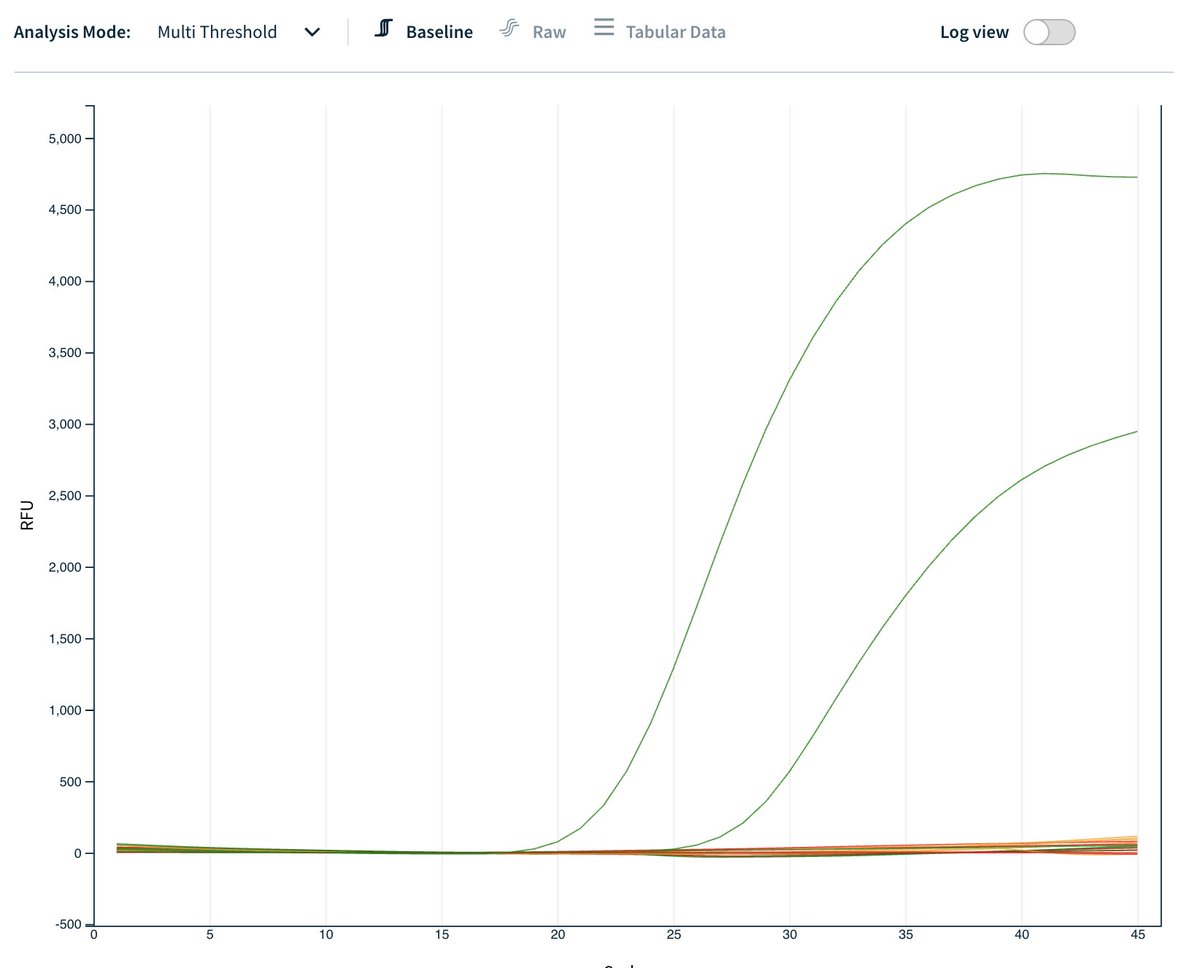
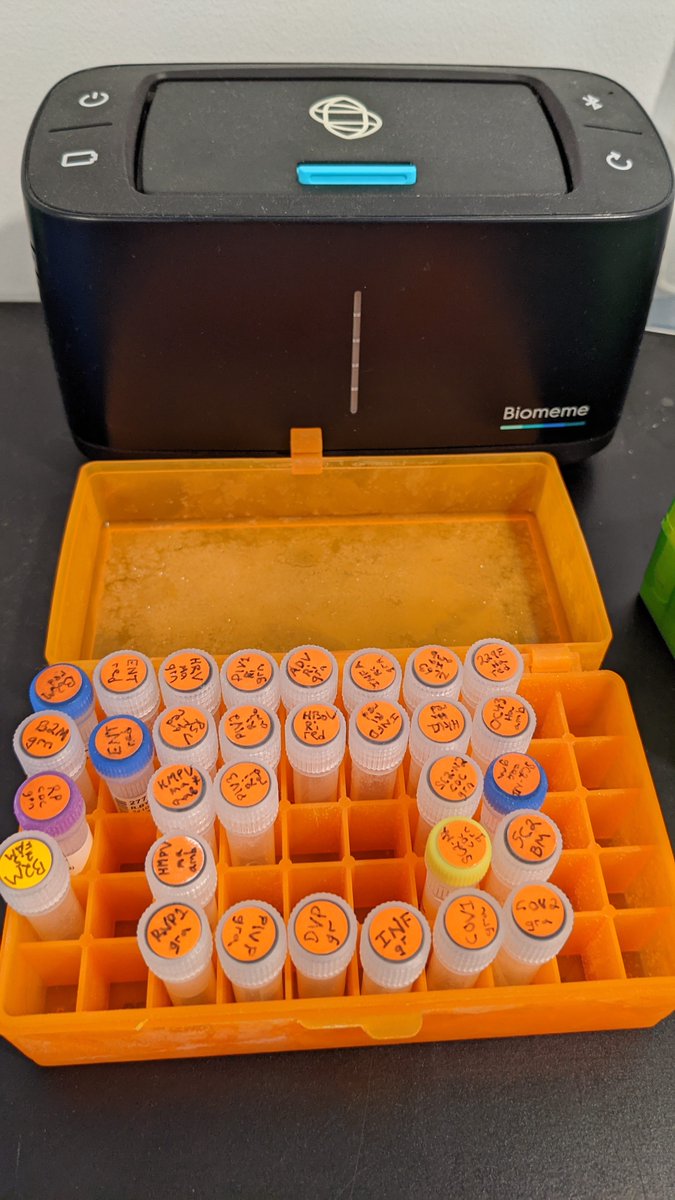
I’m sure most of you are thinking “who cares, it’s not COVID so it’s a cold - what difference does it make if it’s Rhinovirus or Parainfluenzavirus or whatever?”. That’s true, I’m just geeking out on something totally impractical (as the first computer hobbyists did).
For the handful of you who want to geek out along with me, here are the assay details I used: https://docs.google.com/spreadsheets/d/1Unzecg72gMkiTvilp634tVyCdSa6qWtwTcD0QKhtI0g/edit#gid=1750282749
The BEST way to prevent COVID-19 is hand washing? Thanks for the tip, but instead I will teach my kids to look for health advice which cites its sources rather than blindly trusting people comfortable in their position of authority. For example: https://www.theguardian.com/world/2021/feb/14/qa-does-handwashing-stem-the-transmission-of-covid-19 https://x.com/PublicHealthON/status/1449005903710244868
Actually @PublicHealthON, just checking your own sources from 5 months ago would have helped you avoid this incorrect tweet. This document lists hand hygiene last after 6 other mitigations like masking, avoiding crowded spaces, and improved ventilation: https://www.publichealthontario.ca/-/media/documents/ncov/covid-wwksf/2021/05/wwksf-transmission-respiratory-aerosols.pdf?la=en
Hey @michaelmina_lab it looks like the FDA updated their antigen test approval guidelines on Oct 6th: https://www.fda.gov/media/137907/download. There’s a new clause in the asymptomatic evaluation section avoid avoiding participants with recent +PCR. Should help fix the post-infectiousness bias?
I’m thrilled to see this paper finally published: https://dovepress.com/recalibrating-sars-cov-2-antigen-rapid-lateral-flow-test-relative-sens-peer-reviewed-fulltext-article-CLEP.
@michaelmina_lab has been alluding to it in talks for months. It describes how even a perfect asymptomatic contagiousness test would only achieve ~50% PPA relative to PCR. 1/3
Direct comparison to PCR, which is well-known for being positive for weeks or months post contagiousness, has led to a dramatic under-appreciation of the effectiveness of antigen tests for reducing transmission risk. 2/3
Also, is it weird that this paper was accepted in May but only published now, 10 days after Biden announced the new US rapid testing plan and, on the same day, the FDA updated their guidelines potentially addressing the flaw in their approval process? https://www.fda.gov/media/137907/download 3/3
I don’t understand why we’re still having this debate. There’s broad consensus that asymptomatic PCR positives >10 days don’t require isolation. So why on earth would anyone argue that it’s bad for an antigen test to be negative in that same scenario? https://x.com/i_petersen/status/1450940422407266305
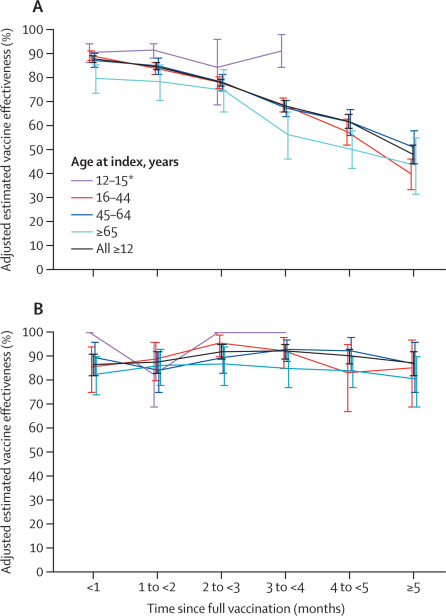
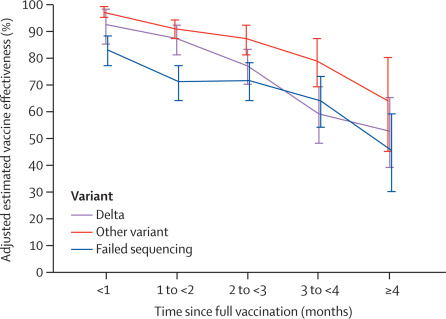
Canada’s 8+ week COVID vaccine dosing interval has resulted in DOUBLE the protection from infection at 4-5 months post vaccination. This is a big deal, real foresight! Those with short interval (often HCWs, elderly) should get boosters sooner. Source: https://covid19-sciencetable.ca/sciencebrief/update-on-covid-19-projections-12/
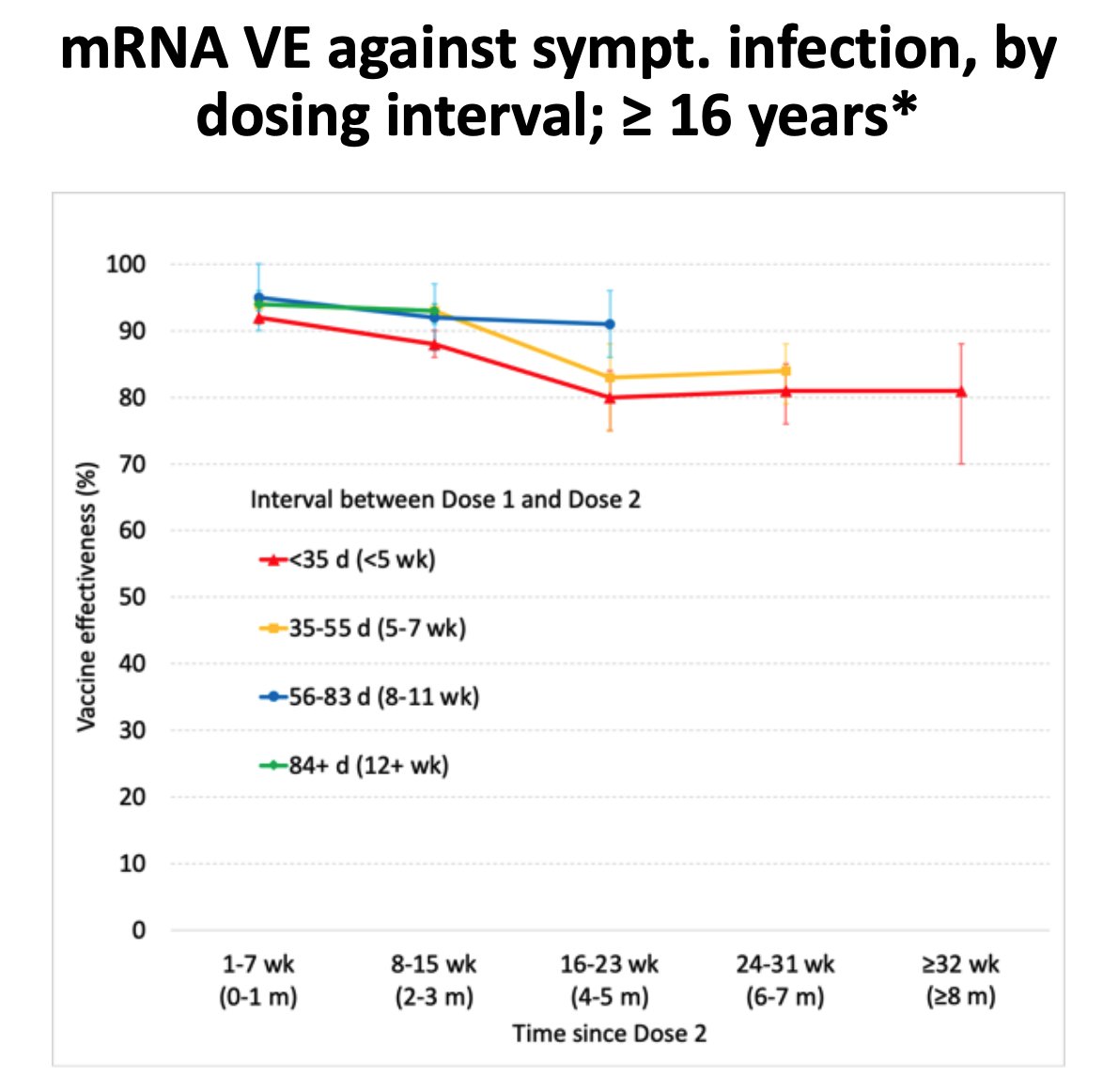
I realized I was sloppy with my wording here. So correction: ”… Resulted in cutting infection risk IN HALF”. VE 80%->90% means infection risk 20%->10%. “Doubling protection” isn’t mathematically accurate. I’m happy to admit when I’m wrong (even without being called out). 😁
It’s great to see Chambers of Commerce distributing rapid testing kits to families instead of just businesses! Will we wait for ICU overload to do this elsewhere in central and western Canada? @OntarioCofC @CdnChamberofCom @My_Chamber https://x.com/C19TestFinders/status/1451562679848550412
Of course I know all to well that this isn’t up to the chambers to decide. We should all be lobbying our provincial government to expand the distribution channel we know has worked for small businesses. Its simple, pragmatic and easily actionable.
The best way to keep our businesses open is to build the capacity for interrupting COVID transmission wherever it’s occuring most. Right now in Ontario that’s kids, not adults! A little paradoxical, but that’s the “public” in “public health”. @CdnChamberofCom https://x.com/RickByersLab/status/1451895898729025551
Yet rapid tests are still used primarily for adult workers, not for unvaccinated children attending schools. https://t.co/vFMY2uEJwi
Finally the US is fixing its regulatory approach to rapid tests, with the NIH helping to “work towards the right benchmarks for performance”. We know people are contagious for less than half the time they’re infected, something current FDA and HC rules don’t seem to account for. https://x.com/michaelmina_lab/status/1452818581062836227
This seems to be why good tests like Abbott Panbio are available in Canada for asymptomatic use only “off-label” in a few provinces.
Encouraging people to eat out caused a “noticable increase” in COVID cases. https://x.com/DFisman/status/1454102488857124864
This is so me 🤓. Except come on @xkcd, using a qPCR machine is SO much more practical than using a sequencer. https://x.com/xkcd/status/1454192525917528068
Another great Dr. Mina interview. This one goes more in depth into the issues with how the FDA is approaching the regulation of rapid tests. This was obviously recorded before the NIH announcement, so I already want to hear another update from @michaelmina_lab. https://x.com/lexfridman/status/1454205894296850442
A great segment with @lexfridman and @NIHDirector on how the NIH is helping to scale manufacturing and accelerate adoption of rapid testing in the US. https://youtu.be/mRZE-SJShkE?t=49m05s
Will Canada be a follower or a leader in North America?
Some great data here. But this fails to ask the key question: is “pausing reopening” alone likely to be sufficient to prevent ICU overload? If not, what more should we be doing? https://x.com/COVIDSciOntario/status/1459192741355786245
With waning immunity (protection from infection only 6x, not 7x anymore), more time being spent indoors and lowering humidity, I fear we’ll have to do a lot more than “pause” to keep from having a disaster on our hands.
I was pleasantly surprised to discover that a third of all know cases are now being sequenced in Ontario. A huge improvement not often discussed! https://x.com/EdTubb/status/1465086438412795911
Unfortunately the data lags by a few weeks, so it’ll be at least a couple weeks before we have a clear idea of how much omicron we have. And we’re still under-testing, so maybe our sequencing coverage is somewhere around 10% of ALL cases.
A great story on @C19TestFinders’ effort to expand access to rapid tests! https://kitchener.citynews.ca/local-news/kitchener-physician-behind-twitter-account-distributing-free-rapid-antigen-tests-4844825
Go Dalia, you rock!
The @COVIDSciOntario brief on rapid antigen screening is out: https://covid19-sciencetable.ca/sciencebrief/rapid-antigen-tests-for-voluntary-screen-testing/
Overall I’m quite pleased with this, and it’s great to have very specific recommendations for usage based on case load. 1/
However, they explicitly use a conservative specificity of 99.1%. StaySafe’s experience with Panbio was consistent with the licensed specificity of 99.8%. I suspect using that number would result in guidance with a much lower threshold (perhaps 75 cases per M instead of 250). 2/
That’s to say: If we use a realistic instead of conservative specificity estimate, then the advice would likely be that most Ontarians should be screening with rapid tests 2 - 3 times per week at today’s case loads!
Millions of rapid tests have been given to businesses to help keep their workers safe. For this omicron Christmas, governments should allow those workplaces to distribute any tests they have sitting around to employees to use with their friends and families. #FreeTheRATs
We’re NOT going into isolation all winter again! The sense of duty was strong last winter, but this winter is very different. Individuals have had every opportunity to get vaccinated and public health leaders have had plenty of time to prepare.
Public health leaders, don’t you DARE ask us to suffer in isolation and educate our kids at home again this winter unless you’re going to show us some basic respect by empowering us with the education and tools needed to gather safely in small groups. #FreeTheRATs
My friends and family are buckling down for a long winter where rapid tests are the only thing keeping us sane.
https://www.levitt-safety.com/pandemic-supply-sourcing/abbott-panbio-covid-19-ag-rapid-test-device/
I’m also worried that rapid test supply could become an issue this winter, time to stock up!
Any students of public health history?
When public health departments in different jurisdictions are fiercely split on the value of a new tool (like self-screening with RATs), which does history suggest is the most probable explanation?
Many public health leaders are:
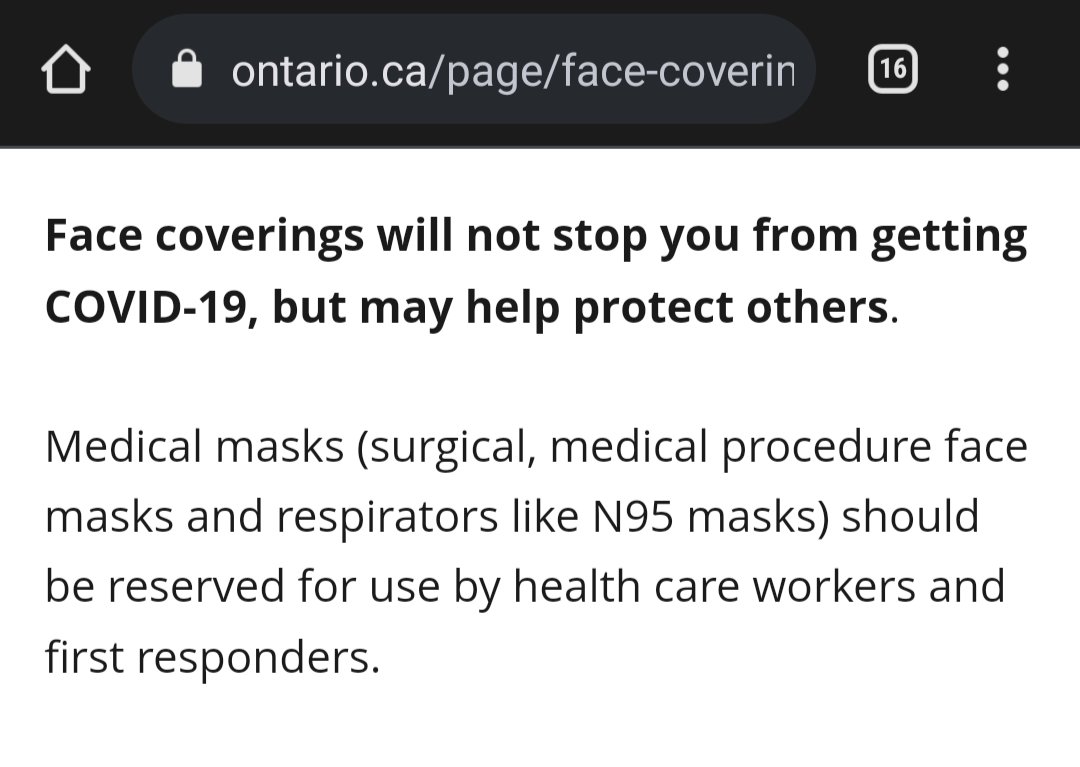
Omicron is bearing down on us, and we still don’t have ready access to 3rd doses or rapid tests. I get it, there are logistical challenges and we again failed to prepare. But how do you explain this @PublicHealthON? Whose science are you following? http://www.ontario.ca/page/face-coverings-and-face-masks#section-0
For all my complaints about Ontario’s handling of rapid testing, giving all students a box with instructions on when to use them is actually quite a solid and bold strategy given the limited supply.
I have optimism for our future (after what will inevitably be a hellish winter). https://x.com/michaelmina_lab/status/1471654368931897349
Yes! Daily rapid tests for contacts would be so much more effective (and less disruptive) than doing a single PCR test! https://x.com/DavidJuncker/status/1471848527475228681
I agree the “I heard ..
from a random person” comments are unhelpful. But I also don’t think “discouraging” this behavior will have any positive effect other than helping our tribe feel more self-righteous. What does research say on how to actually change minds and behaviour?
I know it’s not cool to say “I told you so”, but here’s a draft version of a document I shared with some government leaders back in August: “Population-level rapid testing as a pragmatic alternative to lockdowns” https://docs.google.com/document/d/1QnZ8bpusSbLn4FAivRU6cuV22ngK6X2Lu8Cwy8CIbnY/edit#
In particular, note: “Nova Scotia Public Health has said they see their rapid testing program as a way of normalizing testing for residents so that they have the tool available to deploy at scale quickly should it become necessary. ” 1/
“All too often we wait to act decisively until hospitals are almost overloaded, and then are left with no options other than long and strict lockdowns. Hope is not a strategy.” 2/2
Hearing reports of crowds at rapid test distribution sites. I’d like to remind folks that at http://StaySafeScreen.ca we were giving out over 10,000 tests a day at a single site before the province shut us down.
This is what it looked like.
Source: https://www.therecord.com/news/waterloo-region/2021/10/01/employers-can-get-free-rapid-tests-why-cant-families-get-the-same.html?

We weren’t better equipped, we just had the foresight to prepare and build an awesome volunteer army over a period of months so that we could scale. This is the same reason NS is succeeding while ON is floundering.
Credit where credit is due: Thank you @fordnation for buying 10+ million rapid tests (on top of those from the feds) in time to distribute them for the holidays. That must have been a contentious decision before omicron. I genuinely appreciate the act of leadership. 🙂
I was on CP24 news last night to talk about the great work @C19TestFinders has been doing and the challenge distributing rapid tests. https://www.cp24.com/video?clipId=2346373
Great story. Great quote from @LisaBarrettID: “It’s not to make cases low that you get tested, but to keep cases low”
https://www.macleans.ca/society/ontario-sees-the-value-of-rapid-tests-for-covid-as-ever-way-too-late/
With only 45% of the population using a rapid test at least once, the city of Liverpool saw a 32% reduction in COVID hospitalization compared to regions not using rapid testing.
Just imagine what 100% usage before any gathering could do! https://x.com/profbuchan/status/1472873533873303556
Rapid tests done same-day reduce your risk of gathering by perhaps 10x, roughly the same as a good N95 mask or being 10 days past your 3rd shot. Combine all 3 for a 1000x risk reduction! https://x.com/lisa_iannattone/status/1473461922129494016
I’m grateful for the tests that have been distributed. But 50M over ~6 months is one test per person every 2 months! Think bigger! ⬆️⬆️
I’ve kept my family of 4 safe by purchasing and using over 200 rapid tests in that time. So let’s aim for at least 20x the volume, shall we? https://x.com/fordnation/status/1473436983297032201
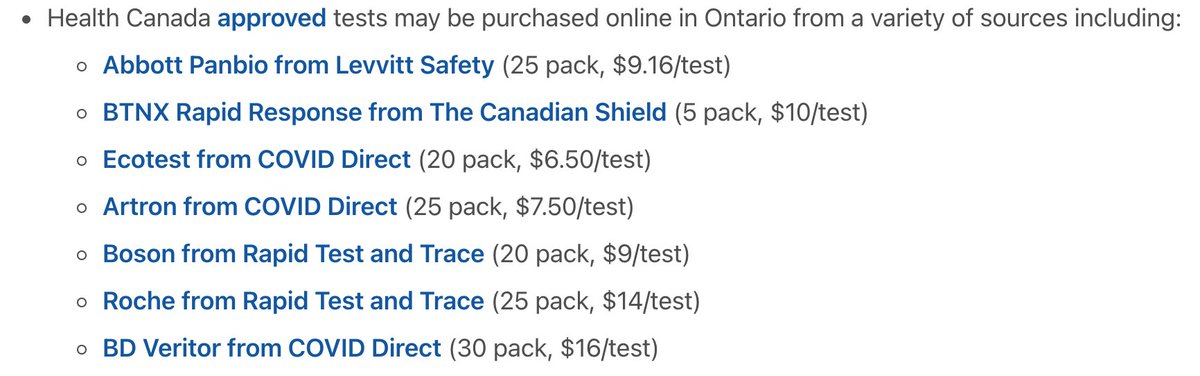
I’ve updated http://StaySafeScreen.ca with a list of all the HC-approved COVID antigen tests I can find available for sale in Ontario with a link to the shop with the lowest price. Let me know if I’ve missed any!
Of course everybody is out of stock until January at this point 😢.
Wow, look at the massive increase in COVID alert keys being generated for Ontario! I’ve plotted both the absolute value (>300 keys/day) and relative to the number of 7-day cases (>10%).
Keep using the COVID alert app. With contact tracing failing it may be your only notice!
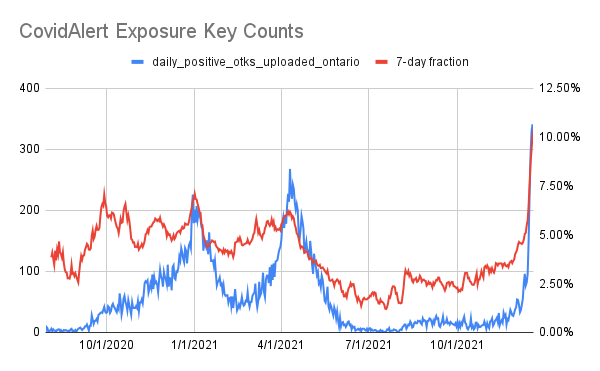
Of course COVID alert is only as good as our testing system and that’s failing too.
I know a high school student who was just contacted by public health to say they were exposed 7 days ago, and that they needed to isolate for the remaining 3 days!
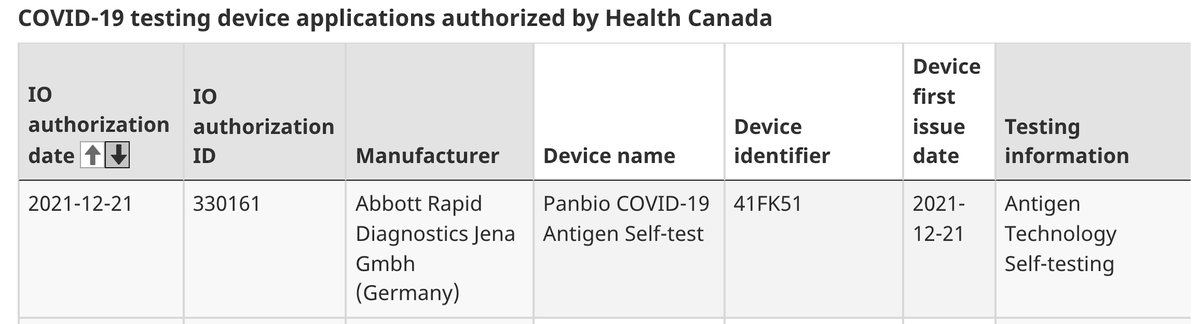
Whoa, look what just showed up on the list of Health Canada approved rapid COVID tests. Finally a company capable of producing hundreds of millions of tests has a license in Canada for a product for consumer use!
Note “PanBio self-test” is distinct from “PanBio”. Cost? 💵😐
Wow, this sounds like exactly what I’ve been dreaming of for years! A home molecular test for a variety of infections. $50/test today but with a goal to match antigen test prices in 6-12 months!
https://www.theverge.com/2021/12/22/22849030/covid-test-detect-startup-meta-google
Wastewater data from Waterloo region suggests we’re missing an awful lot of COVID cases right now. 😢 Be extra careful folks, there’s a lot of unidentified Omicron out there!
https://www.regionofwaterloo.ca/en/health-and-wellness/covid-19-wastewater-surveillance.aspx
A great resource clearly explaining the science and mitigations for gathering this holiday season. It handles the nuance around usefulness of rapid tests well. https://x.com/COVIDSciOntario/status/1474177734628847618
A great anecdote, suggesting that doing oral-nasal swabbing is perhaps worth it. I don’t see much downside since it’s been validated by some labs like Michael Garron Hospital. So I’ll probably start doing this myself. https://x.com/obenfine/status/1475252837177348100
Instructions: https://youtu.be/5qHTBlxfNes
Note that Panbio is approved for throat+nasal swabbing in Ontario. I highly reccomemd it. https://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/Antigen_Screening_Guidance_2021-03-5.pdf
Thanks @DrKateTO for pointing this out! https://x.com/obenfine/status/1475252837177348100
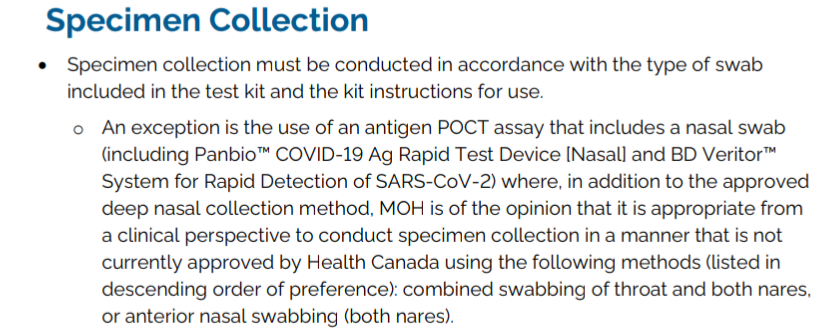
Again, the UK has good instructions since they’ve been doing this swabbing technique since the start: https://youtu.be/5qHTBlxfNes
Interestingly, the benefit might be from collecting saliva. More data needed! https://www.medrxiv.org/content/10.1101/2021.12.22.21268246v1
Wow! So who will be the first to build an open source app to automatically generate viral load plots from LFT photos? https://x.com/methanoJen/status/1476276591219064836