
Open source decentralized vaccine development… Interesting 🤔 https://x.com/HoekstraTweets/status/1463294339296206862
Post Archive 2022
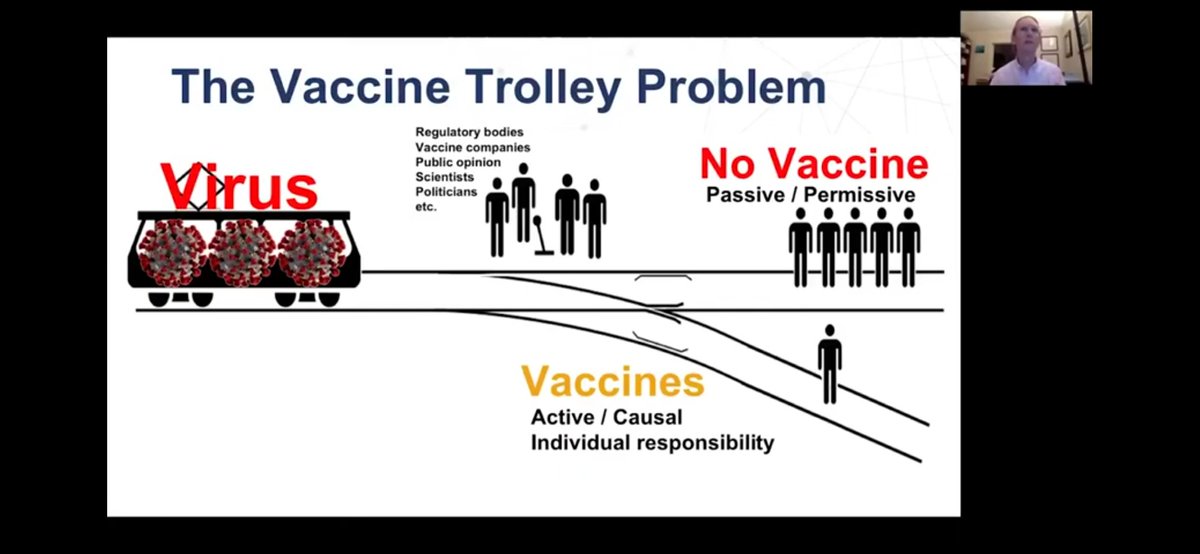
Wow, I won’t pretend to have the answers but it’s hard to believe that the questions being raised by @RADVACproject aren’t getting more serious consideration and widespread discussion. https://youtu.be/1Tzj76m1n1A
If you were the one standing at this switch, how quickly would you pull it? I’m glad I’m not standing there. But perhaps that’s the problem - we’d all rather share responsibility for millions of preventable deaths than risk personal blame for a few.
I know it’s just an anecdote but I keep thinking about this fascinating story. I think it’s far more likely that @HoekstraTweets has prevented rather than caused harm to himself (and possibly others) by self-experimenting with a COVID vaccine. https://x.com/HoekstraTweets/status/1473381904707633153
12 years ago most experts felt it would be reckless to update major web browsers more often than 6-12 months. Now 4-6 weeks is the norm.
It’s far from a perfect analogy, but perhaps there’s something to learn from this for vaccines? @RADVACproject https://radvac.org/ 1/11
- Chrome led this “evergreen browser revolution” by taking the controversial position that it was more important to be able to respond to issues very quickly than to have maximum confidence in quality before releasing. A fast update culture can reduce net harm. 2/11
- Updates happen in a staged fashion with careful attention to usage and performance metrics. If there’s an anomaly we can’t explain, updates are paused (or, worst case, recalled) while we figure it out. 3/11
- Lab testing is of course still critical. We do as much as we reasonably can WITHIN our release timeframe. 4/11
- Rapid and tight feedback loops are essential. If something goes wrong, users can file bugs with a system in place such that the right developer can hear about it, and potentially take immediate corrective action. 5/11
- The Chrome team created a culture and set of processes to ensure that emergencies would be dealt with effectively in a matter of hours. This includes “blameless post-mortems” to constantly get better at emergency response. 6/11
- Risky changes are done as random A/B trials starting with a small population and ramping up only when metrics look good. Yes, that means Chrome is always experimenting on average users and some users are harmed as a result! 7/11
- All users are given the choice to opt-in to even higher risk models (daily-update canary channel, weekly update dev channel, etc.) and feedback from those populations are essential to decision making for the larger user population. 8/11
- Finally, Chrome was released open source as the Chromium project so that when we inevitably make mistakes or have blind spots, others can step in and correct them by competition (forks) and/or cooperation (upstream contributions). Users can choose more stable browsers. 9/11
Ok, I know you’re outraged that I’m suggesting maybe doing things with vaccines which would cause some harm. The important question is how much more or less harm than status quo?
Millions died while we waited for COVID vaccine trials! https://www.youtube.com/watch?v=1Tzj76m1n1A 10/11
Oh and if you think this fast-update model can’t possibly work for something with life-and-death consequences, then you probably don’t yet own a Tesla. It’s just a matter of time before most cars will follow this “evergreen” model too. 11/11
This is exactly right! Most people don’t realize that Health Canada has been dolling out millions of tests for almost a year now for a use case that Health Canada has not authorized and relies on the provinces to overrule! Dr. Jekyll and Mr. Hyde indeed! https://x.com/DavidJuncker/status/1479198828200927238
There’s now a larger fraction of under 5s in hospital with COVID than any other age group under 60. Ignoring those still ineligible for vaccination is unethical. https://www.publichealthontario.ca/en/data-and-analysis/infectious-disease/covid-19-data-surveillance/covid-19-data-tool?tab=ageSex
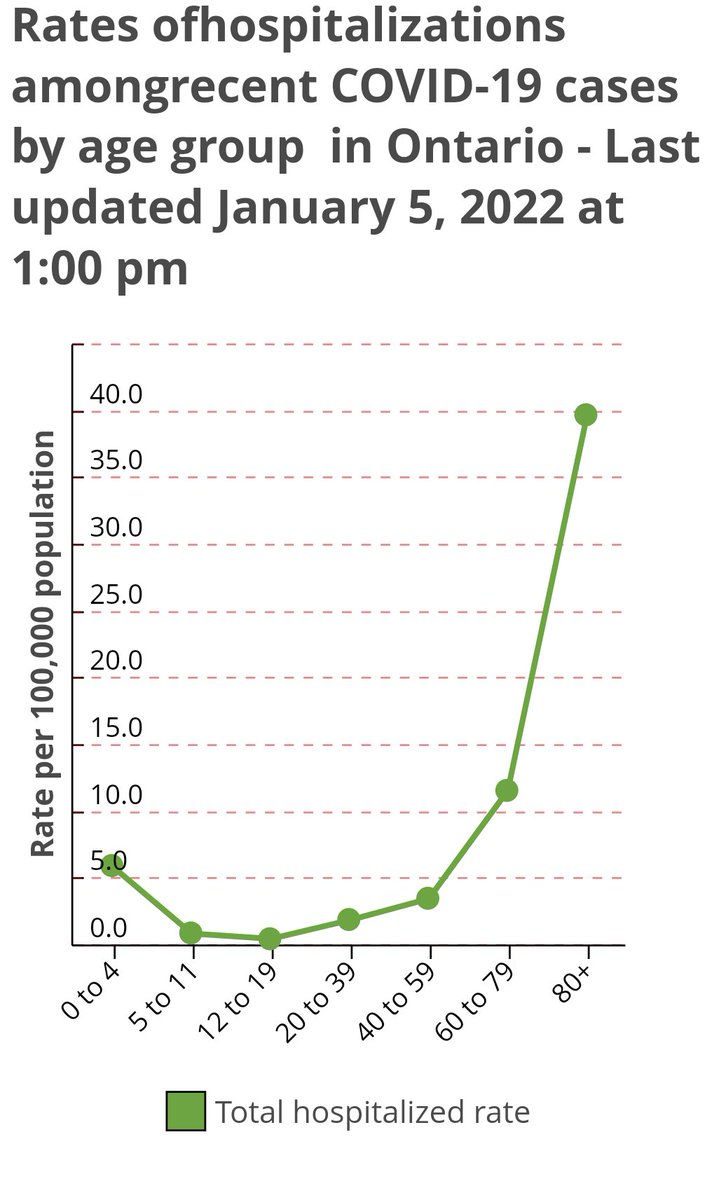
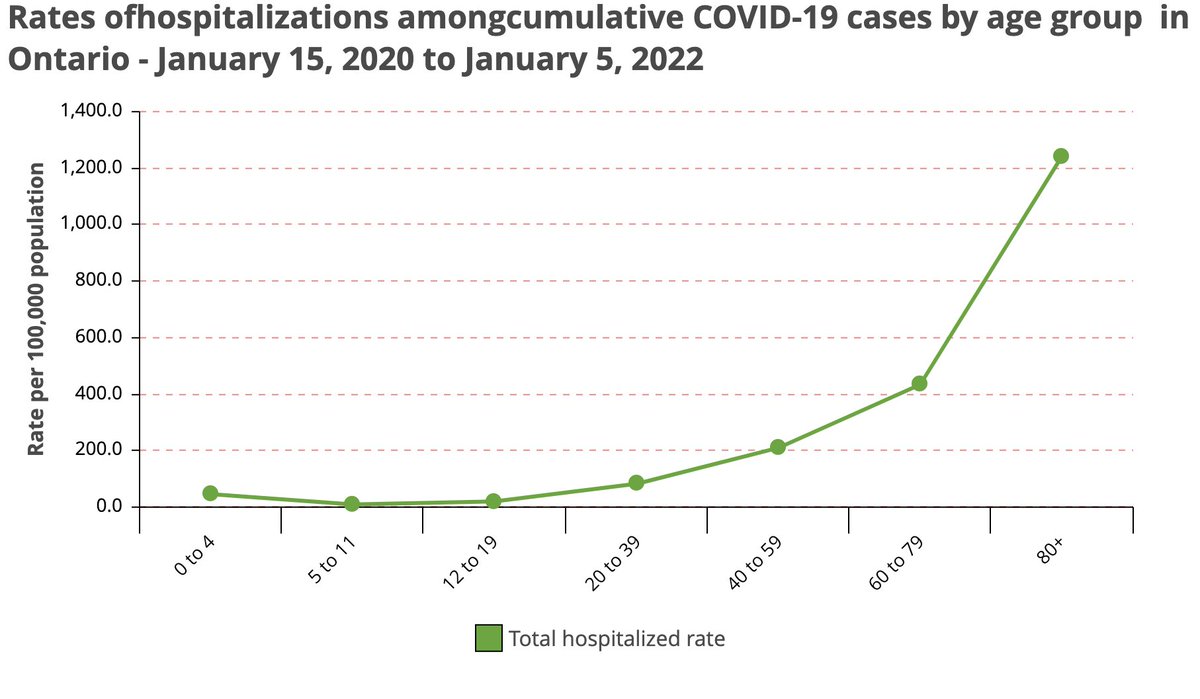
Note that something has gotten much worse in the past two weeks. Compare to hospitalization rates throughout the pandemic. 13% of all children <5 who have been hospitalized with COVID have been hospitalized in the last 2 weeks, compared to 3% for all age groups combined. Omicron?
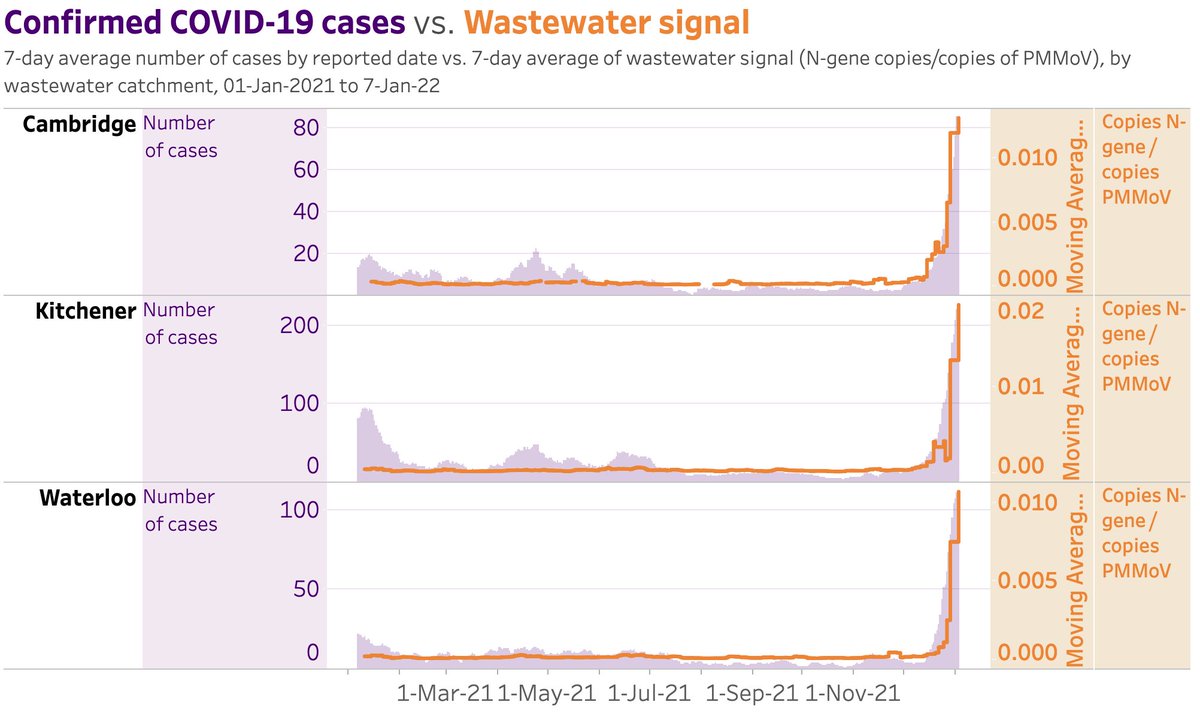
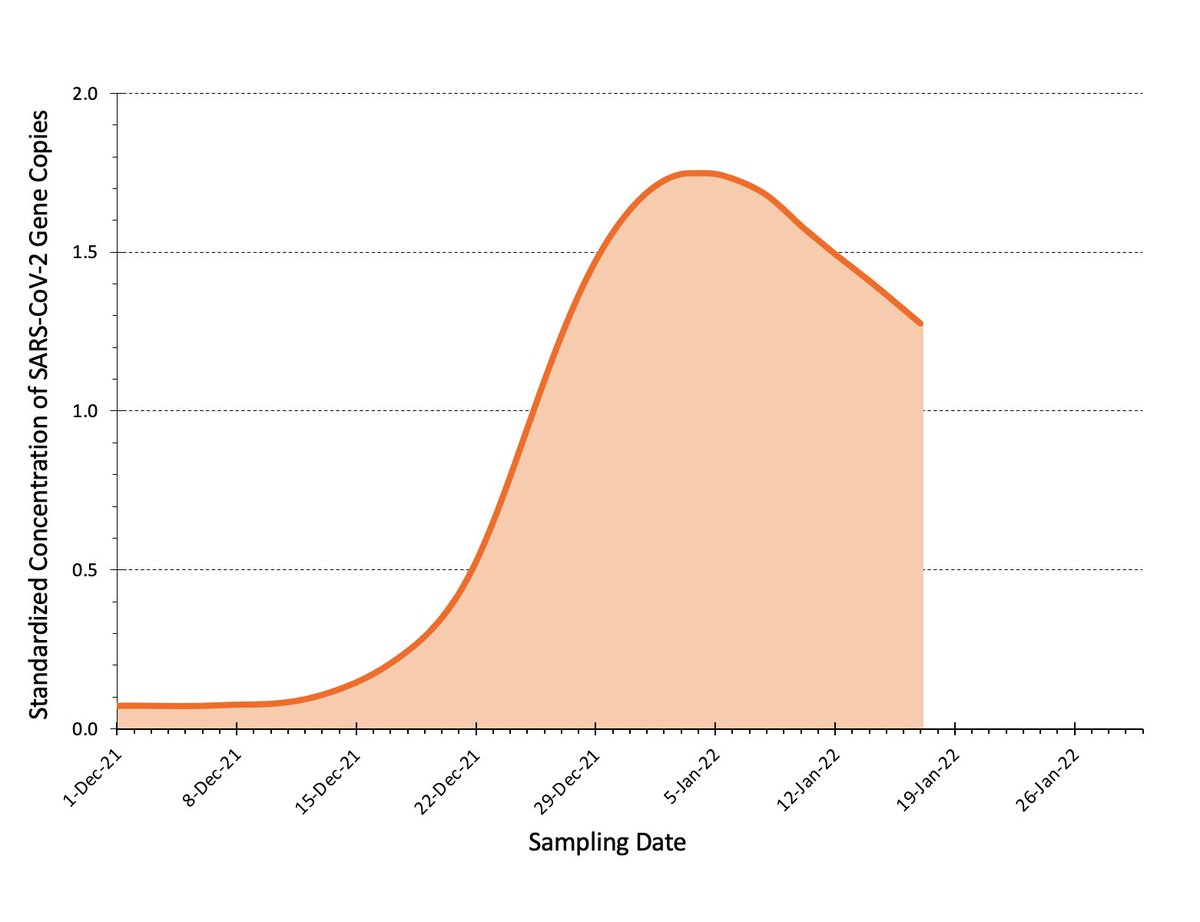
A new batch of wastewater data is out for Waterloo region. As expected the signal has surged well above any level seen previously. I’m surprised however that PCR-confirmed case counts are keeping pace. This is only up to Jan 3, so I expect a greater disconnect next week. https://x.com/RickByersLab/status/1474012436399370243
Earlier this week I emailed a rapid testing expert to ask if they had data on throat vs. nasal swabbing. They told me no but they had symptoms themselves for the past two days but had tested negative in the nose. They did a throat swab and it was positive! Another nasal was neg.
I know it’s too small of a sample, but that makes two of two people I’ve asked getting throat positive at least a day ahead of nasal. Its highly unlikely this is coincidence.
Hey FDA, you’re still of the opinion it’s desirable for antigen tests to be positive in the long post contagious period like PCR tests are, right? You’re just digging yourself further into the lack of credibility hole here… https://x.com/US_FDA/status/1479548116684709890
It feels like we, as a society, have been given 2 years to learn and practice infection control, and now we’re all being put to the test. Trial by fire! How are we doing?
All of Ontario Twitter seems outraged by the disinformation in this tweet. Never mind that the official PHO website STILL says we should not be wearing respirators or medical masks AT ALL! The longer this lasts the funnier it gets! 🤣😥😂 http://www.ontario.ca/page/face-coverings-and-face-masks# https://x.com/PublicHealthON/status/1481269754409144321
Family of mine in Ottawa tell me many there have been following wastewater COVID trends for many months like the rest of us follow weather forecasts. All of Canada should have this ability and awareness! https://x.com/RickByersLab/status/1482720643221233670
Agreed! Vaccines are great but pretending they’re great for things they’re currently quite poor at just erodes trust! People are smarter than this! Bring on the Omicron boosters so we can claim this once again! https://x.com/uhwuhna/status/1483903247203147780
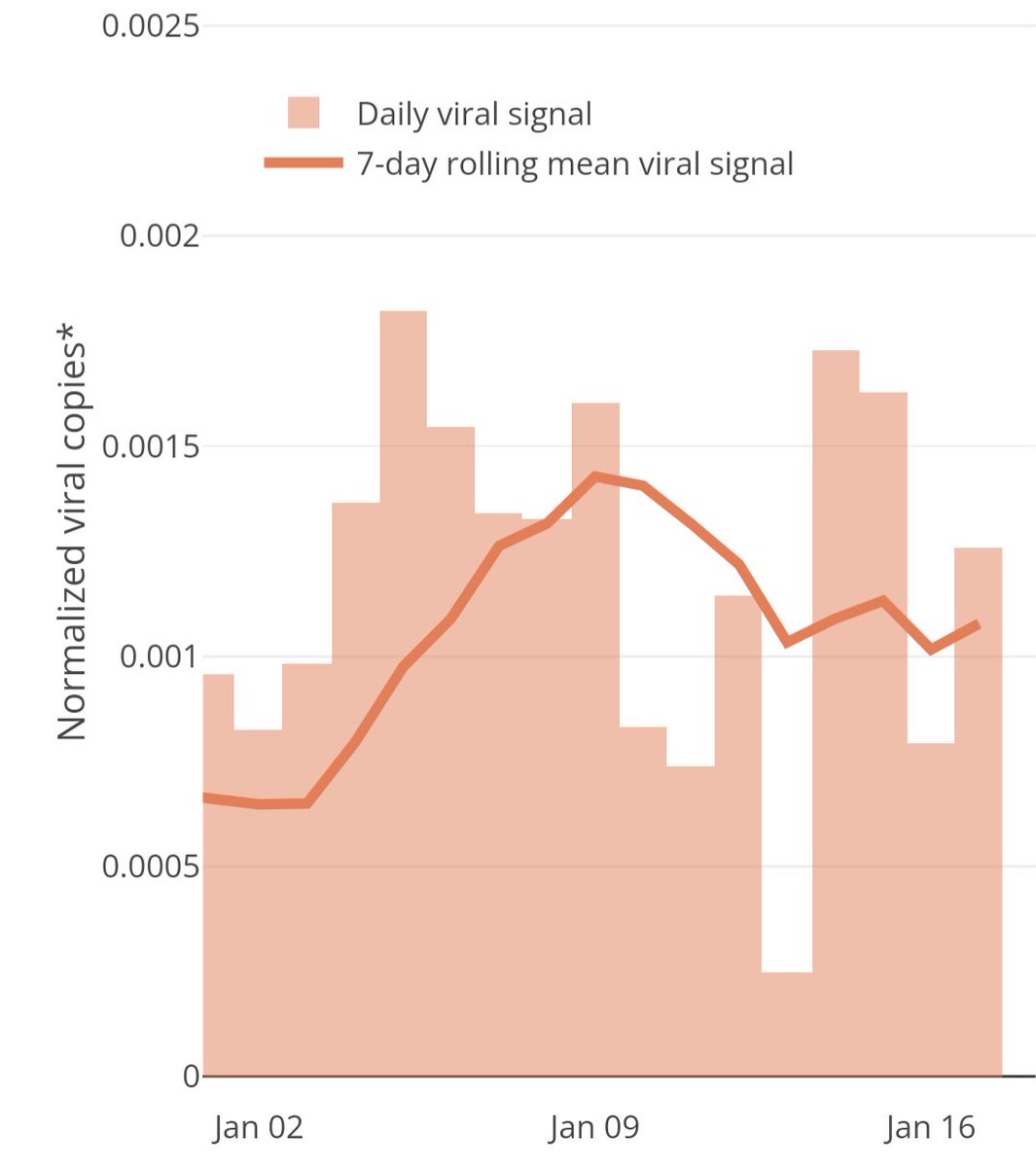
Ottawa wastewater data is the best signal we have into COVID prevalence in Ontario. After being optimistic for a few days, I’m now quite confident we’re not seeing the dramatic drop in prevalence many are claiming.
https://613covid.ca/wastewater/
Great to see some hard data on this! Based on many anecdotes I’m surprised there’s not more gain w/ Omicron, but I’ll take preprint data over random anecdotes any day! https://x.com/Bob_Wachter/status/1484316590715723776
But this data from Nova Scotia Public Health suggests that adding the throat does offer a significant increase in sensitivity: https://www.cbc.ca/news/canada/nova-scotia/ns-combined-nose-throat-rapid-test-more-accurate-1.6322961. Given their great track record on rapid testing, I trust NS public health!
It’s great to see a steady increase in the number of COVID rapid antigen tests approved in Canada! Hopefully this will soon translate into greater supply and lower prices.
https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/medical-devices/authorized/list.html
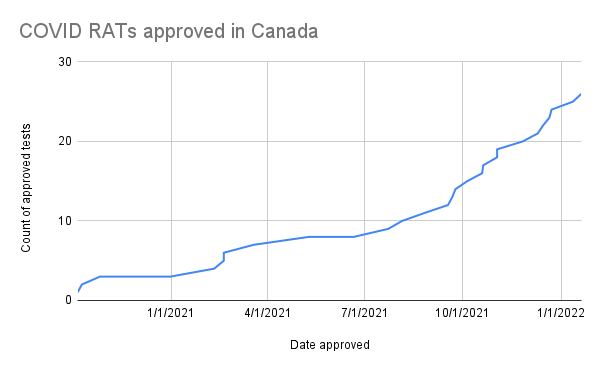
Of course we still have a long way to go to catch up to Germany, who has approved 592 rapid COVID tests! https://antigentest.bfarm.de/ords/f?p=110:100:17541466902457:::::
Wow what a simple, clear and effective website from the US government for obtaining free rapid tests: https://www.covidtests.gov/. If only things could be this straight forward in Canada!
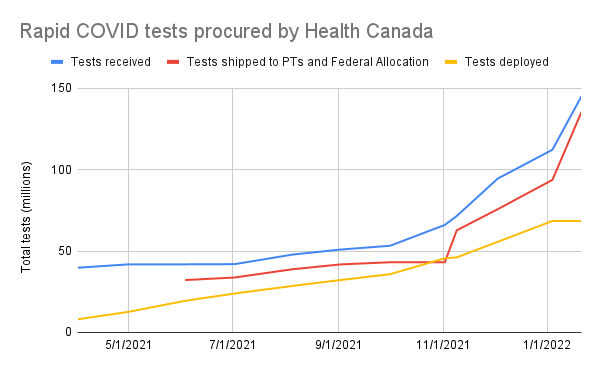
As expected, there’s been a good acceleration in the total rapid tests procured and distributed by Health Canada. But why are “tests deployed” lagging so much? From historical snapshots of https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/testing/increased-supply.html
How each province has taken advantage of the Government of Canada’s rapid COVID test program relative to their population.
Source: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/testing/increased-supply.html
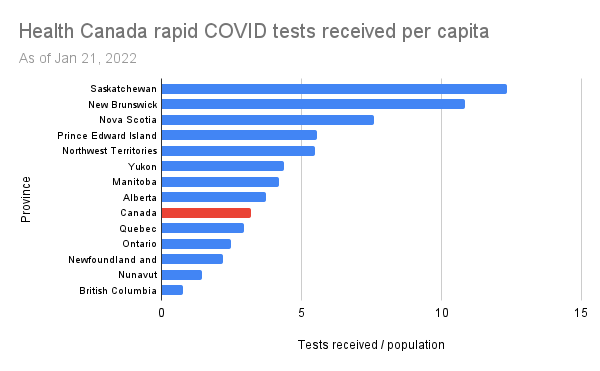
Note that some provinces, at least Ontario, have also procured millions of tests on their own and so this is just a lower bound on the availability of government funded tests in each province.
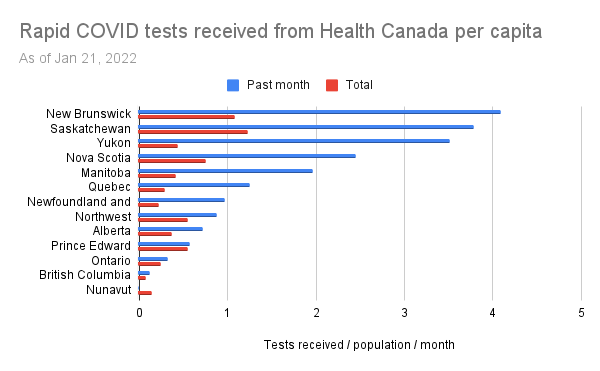
It looks a little different if we look at only the tests received over the past month (when the value has been hard to deny). It looks like some provinces have really stepped up their requests, while others have not.
Raw data: https://docs.google.com/spreadsheets/d/13ReJ4LycRmy2fBm7DkKeddzErXf92SIXfRAD7HGKtA4/edit#gid=1189947003
Comparing Canada and USA for rapid test approval. What changed in the USA on Oct 21, 2021 and how can we effect a similar change in Canada?
USA Source: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas-antigen-diagnostic-tests-sars-cov-2
Canada Source: https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/medical-devices/authorized/list.html https://x.com/RickByersLab/status/1484634454568189964
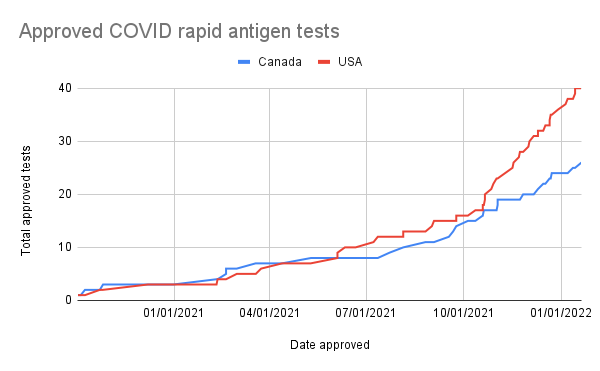
I’m guessing it has something to do with this: https://www.nih.gov/news-events/news-releases/nih-radx-initiative-expands-covid-19-testing-innovation-additional-types-rapid-tests
Throat+nasal swabbing significantly more sensitive than nasal alone in both Panbio and BTNX.
I was worried that the NP swab that comes with the BTNX kits wouldn’t work well in the throat, but it seems not to be an issue! https://x.com/DavidJuncker/status/1485024750741213185
. @COVIDSciOntario has updated their excellent dashboard to include a province-wide wastewater signal. This looks a lot smoother than the per-region graphs I’ve been following. Now if we could just get the latency down a bit lower than 6 days. https://covid19-sciencetable.ca/ontario-dashboard/#wastewatersignal
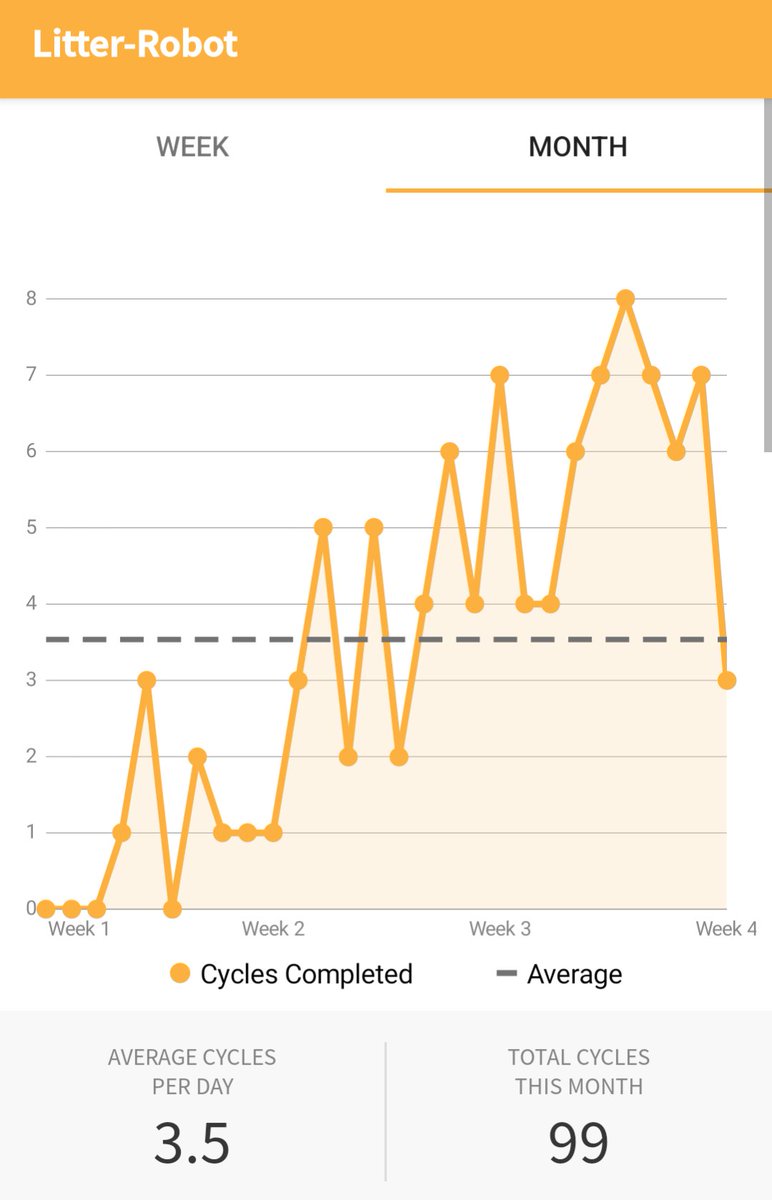
Since you all seem to like when I post graphs of interesting data, here’s another one for you.
“It’s as easy as that, get your COVID test at home for free”. Common Canada, you may not be good at innovating faster than America but you’re at least a good follower! https://x.com/POTUS46Archive/status/1487171196781215753
In the future, when we have outbreaks vaccines will be mailed to every house (eg. in nasal form). When new variants arise, we will test and update our vaccine formulations within weeks. Wastewater testing will mean the right vaccines will be sent to the right places quickly.
Most people will take these vaccines and rarely feel the need to alter their behavior otherwise. We’ll look back on our failure to handle pandemics like COVID-19 like we now look back on sailors who struggled with scurvy due to lacking simple vitamin C supplements.
This may sound like sci-fi, but it’s not really. We probably have the capacity to build up the technology today. So much physical and economic suffering due mainly to a lack of vision and willpower. 😢
https://RadVac.org @RADVACproject
True, but it took over 50 years from the invention of seatbelts for them to be mandated in Ontario (8 years after the USA). Still many believed they were safer without them. Apparently we are terrible at adopting life saving tools when they involve the slightest inconvenience! https://x.com/DrShaneRRR/status/1489339895768555523
“Our clusters abated rapidly compared to previous reports of hospital-based SARS-CoV-2 clusters”
So, hospitals can significantly reduce infections of patients and staff with good masks and rapid tests? Shocking! 😉 https://x.com/C19TestFinders/status/1491020376545333249
Thank you @celliottability and @fordnation for providing widespread access to rapid tests in Ontario. This program looks awesome.
I have nothing snarky to say in this tweet, credit where credit is due… https://x.com/C19TestFinders/status/1491442923455803392
@COVIDSciOntario strongly recomends the use of throat swabs, regardless of manufacturer or swab type! Their instructions: https://www.youtube.com/watch?v=b09cG9wdzdM https://x.com/COVIDSciOntario/status/1491761564378185740
When comparing test sensitivities it’s critical to use a calibrated viral load cutoff like 10^6 RNA copies/ml. Ct values themselves are almost meaningless. Here’s why with an example:
1/8
I was researching the sensitivity of the Innova rapid antigen tests used widely across the UK. Low viral load samples need to be ignored because they generally don’t represent contagious levels of virus. Many studies use a PCR cutoff around Ct<25.
2/8
The big Liverpool Covid-SMART study showed a sensitivity of 69% at Ct<24. Kinda poor. https://www.bmj.com/content/374/bmj.n1637.short
3/8
But then I checked this German survey of tests and it found a sensitivity of 94% at Ct<25. https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.44.2100441#html_fulltext But that’s based on a much smaller sample size than the Liverpool study. Is it just wrong?
4/8
No! Ct values are relative to a particular device and test protocol (eg. A sample diluted 2x more will have a Ct one higher). Sadly most studies don’t publish their Ct calibration in absolute terms like RNA copies per ml. But these two do!
5/8
German study: Ct=25 is 10^6 RNA copies/ml.
Liverpool study: Ct=24.4 is 10^4 RNA copies/ml.
That’s a 100x fold difference!
The Liverpool study uses Ct=18.3 for 10^6 RNA copies/ml.
6/8
And sure enough at Ct<18.3 the Liverpool study shows a sensitivity of 91%, exactly consistent with the German study!
7/8
So in conclusion, don’t trust any test sensitivity number unless it’s accompanied by a cutoff in terms of RNA copy number.
>10^6 RNA copies/ml is a good standard threshold for contagious samples.
8/8
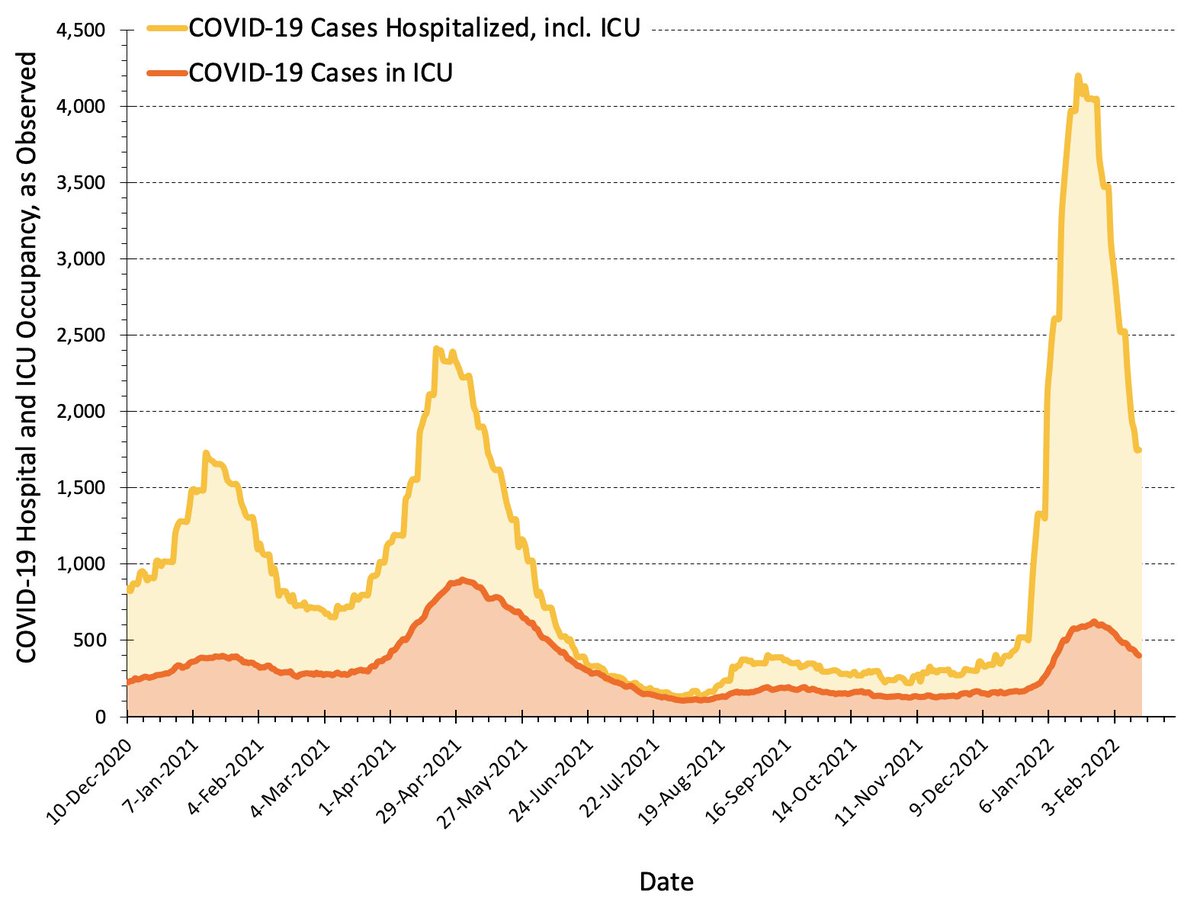
@fordnation says “Given how well Ontario has done in the Omicron wave we are able to fast track our reopening plan”. I’d love to know what metrics of success our government is using. Here’s the main metric I’m watching. https://www.thestar.com/politics/provincial/2022/02/14/ontario-moving-up-reopening-dates-vaccine-passports-gone-as-of-march-1.html
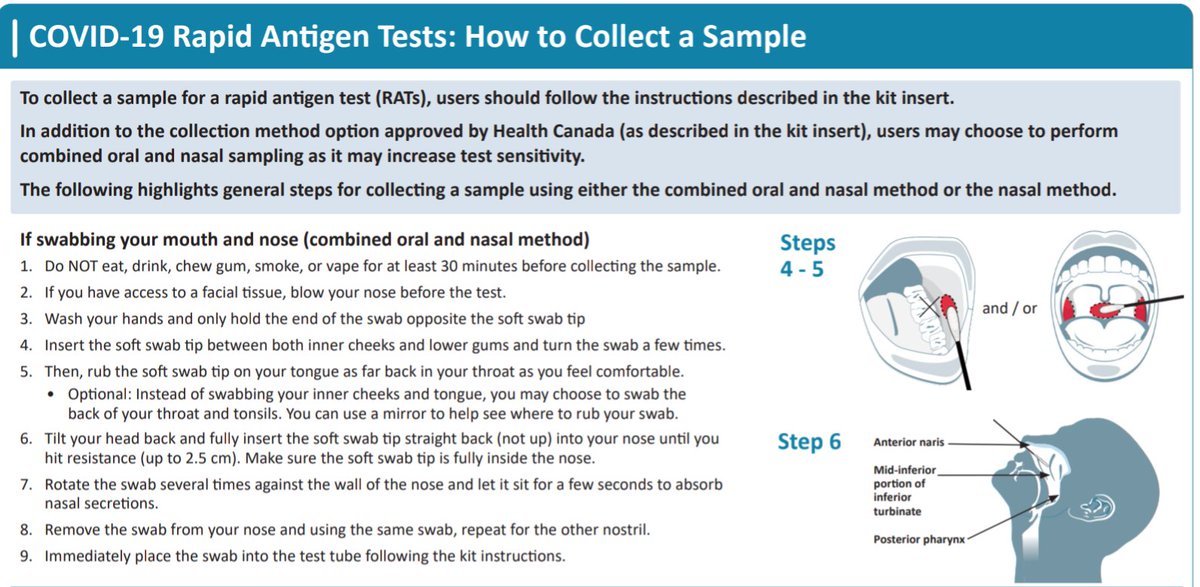
Hurray, Ontario Health endorses throat+nasal swabs for rapid testing! Kudos for being on top of the evolving science! https://www.ontariohealth.ca/sites/ontariohealth/files/2022-02/COVID-19RapidAntigenTests-HowtoCollectaSample.pdf
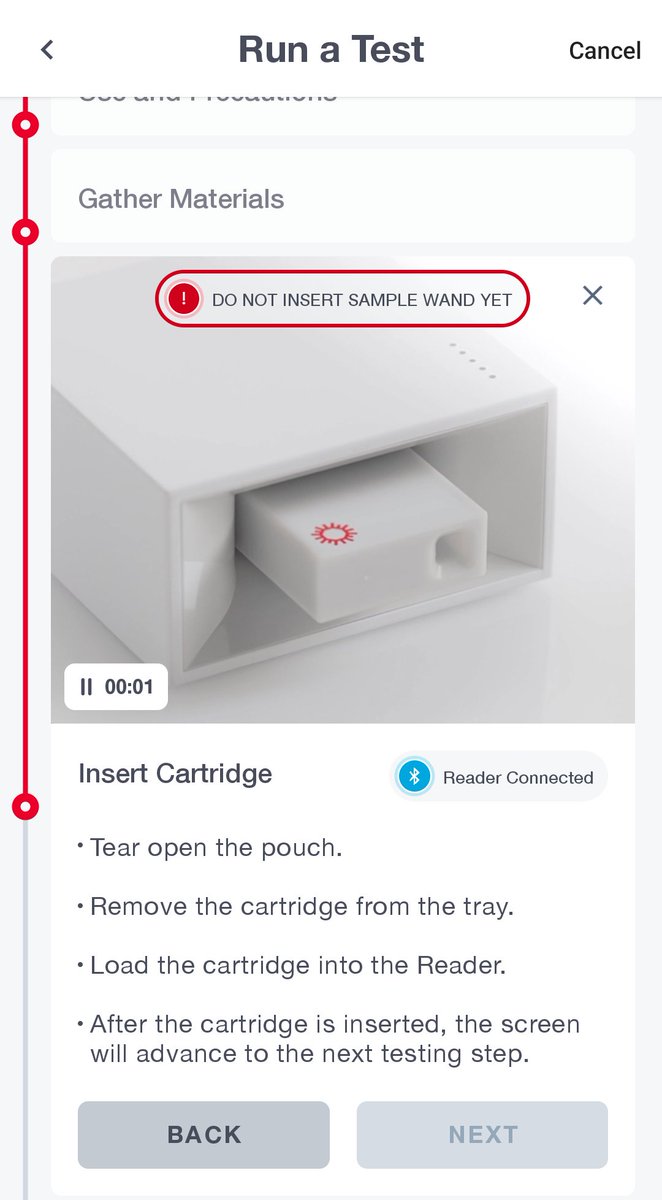
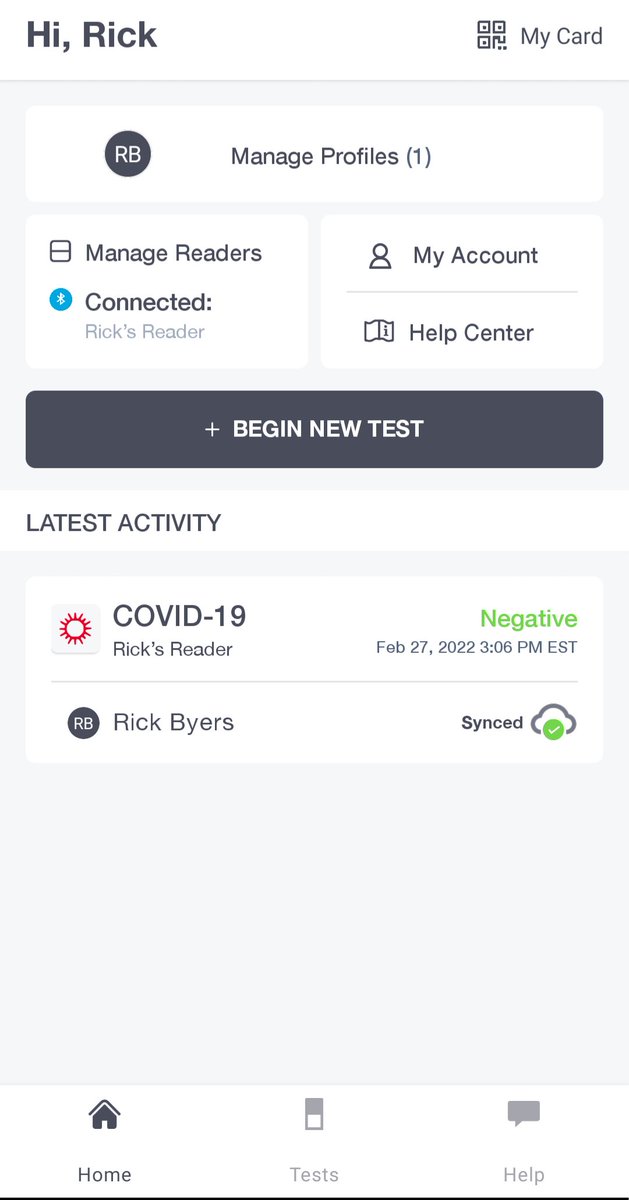
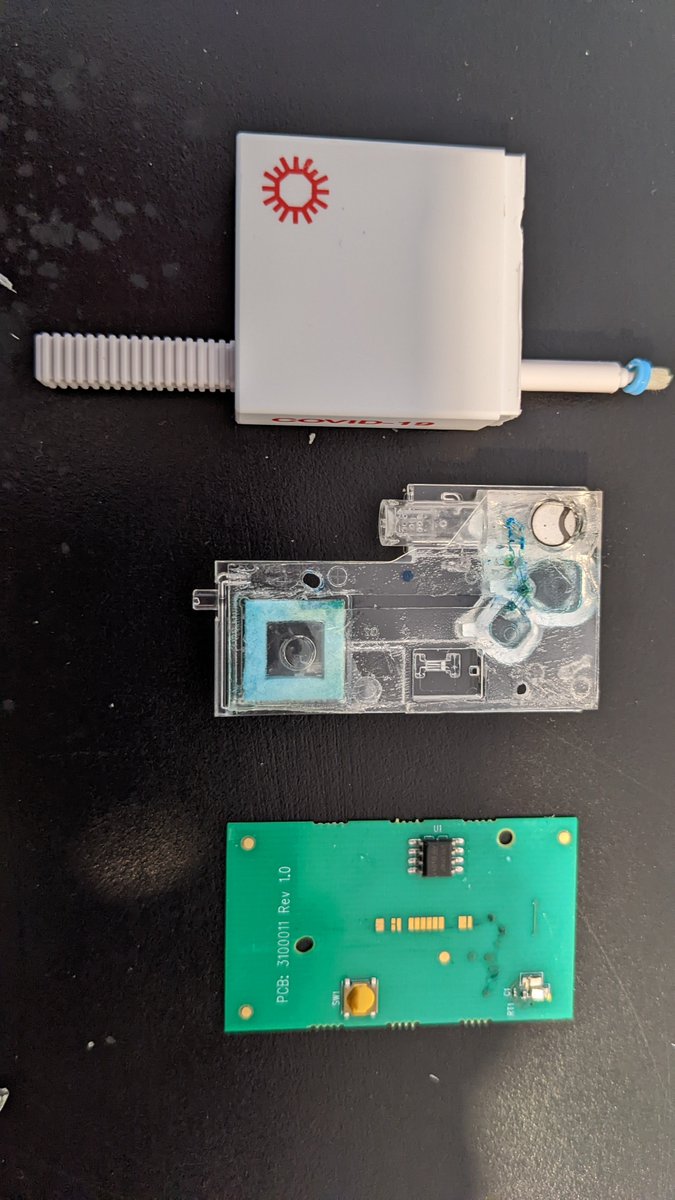
I finally got my hands on a Cue rapid COVID test device: https://shop.cuehealth.com/pages/all-products. Here’s a brief analysis and mini teardown:
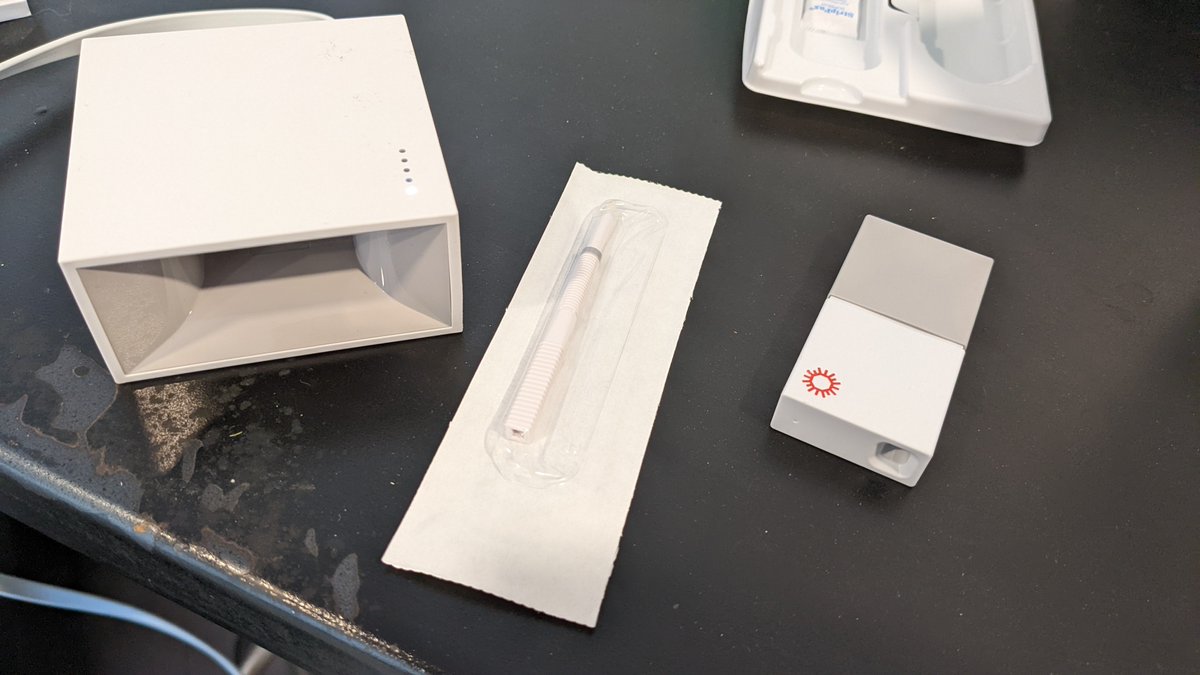
The Cue is a molecular test similar to lab-based PCR tests and the Lucira check-it. They’re more sensitive than antigen tests, but at >$60 per test, for screening purposes you’re probably better off doing antigen tests 3x as often for half the price. Still, it’s interesting.
There is a nifty app that controls the device and walks you through the process.
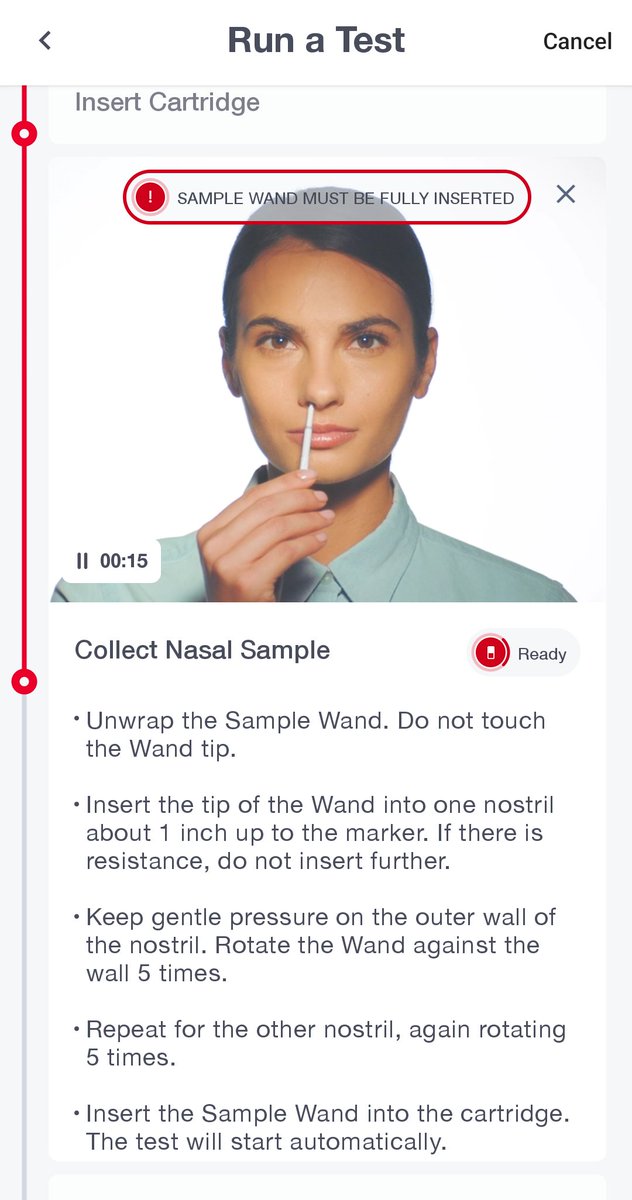
Results take about 15 minutes.
The cartridge itself seems pretty simple, giving me hope that at scale perhaps they could be a lot cheaper. In 2014 they claimed Flu tests could cost about $10 each: https://www.theverge.com/2014/6/13/5801022/cue-hopes-to-be-your-portable-personal-health-testing-lab

It looks like there’s only a single reaction chamber with some sort of electrical sensor that sits above the heater in the reader. Fluid flows from two chambers, through the swab and into a sponge.
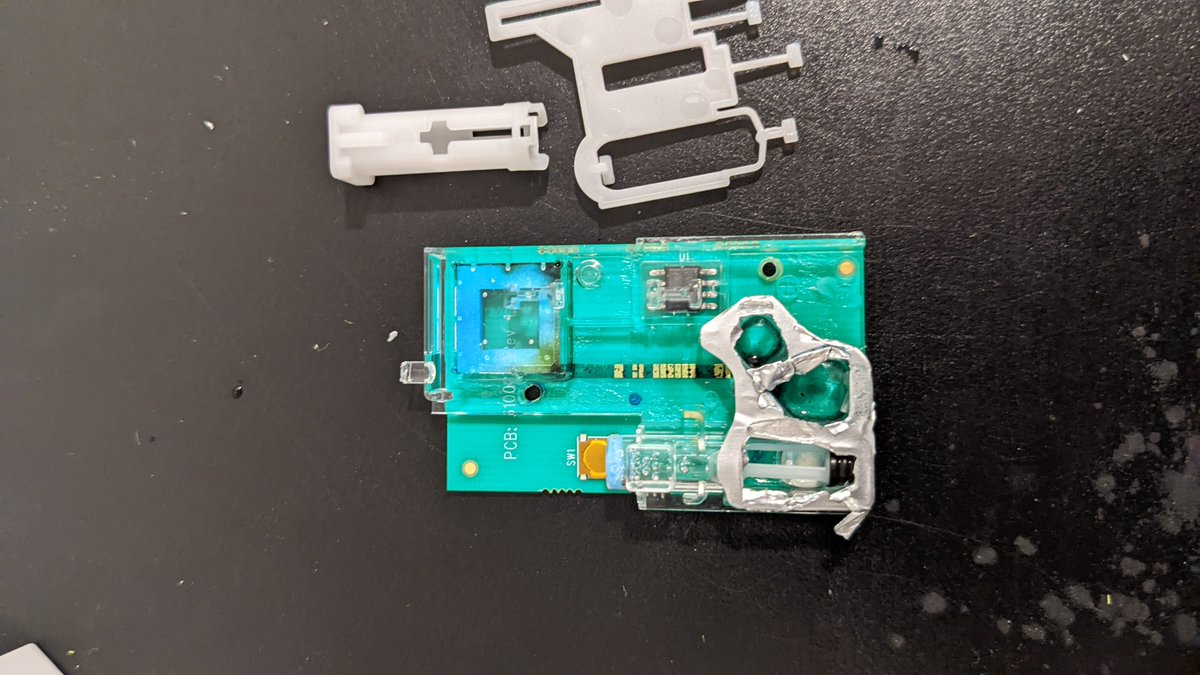
This is a fair bit simpler than the Check-it which has 8 reaction wells and a camera to watch the colour change. https://x.com/RickByersLab/status/1431076518579552260
I’m guessing it’s also RT-LAMP but with some sort of electrical measure of the pH change. But it claims to also test for human RNaseP, so a swab without a sample will return invalid. I have no idea how they’re obtaining multiplexing in one reaction well with no optics. Thoughts?

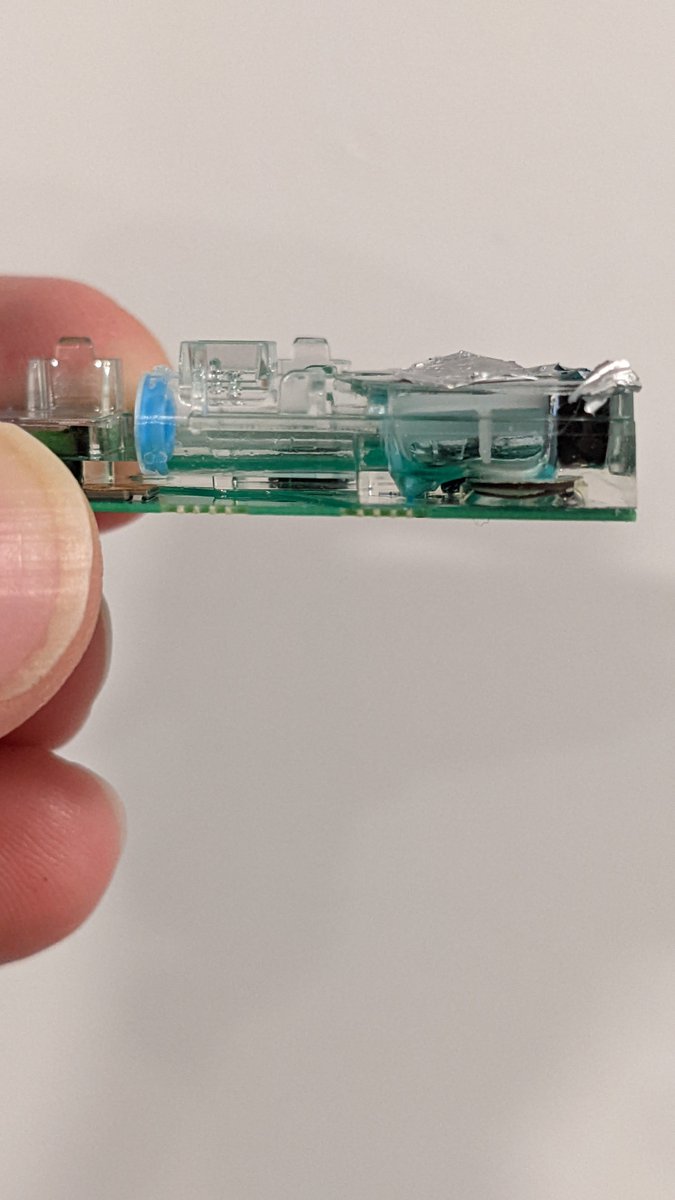
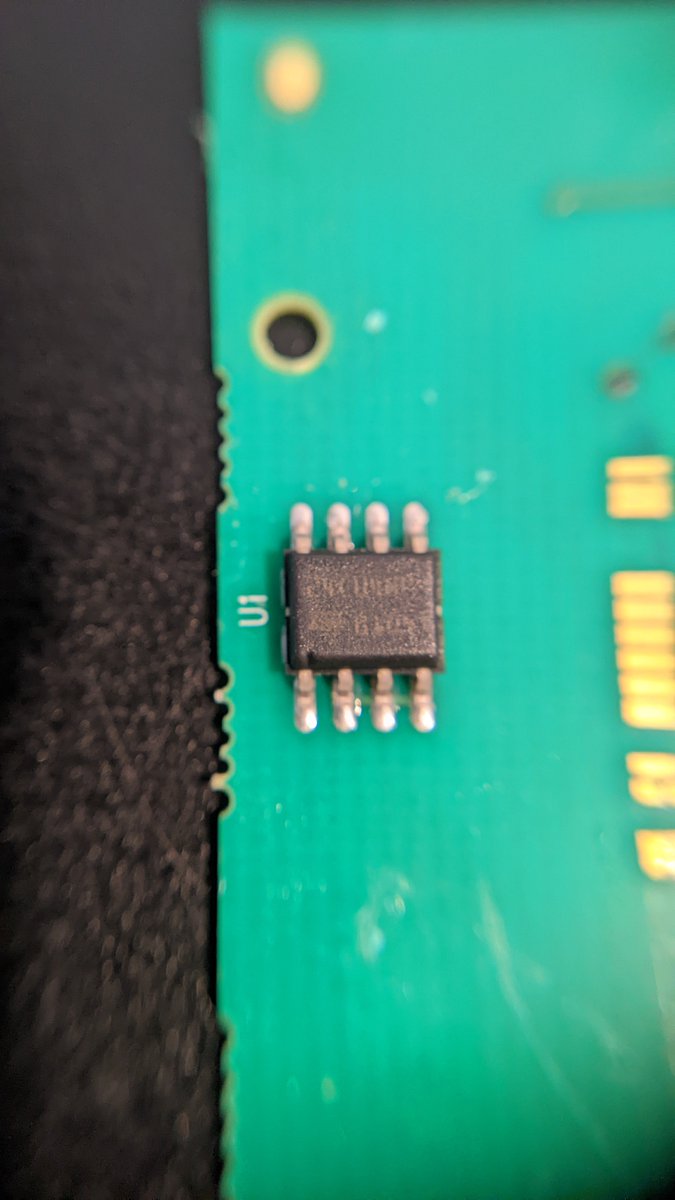
I managed to pry it apart further. The chip looks to be a 24C04, 4kbit EEPROM worth about $0.32 USD. So probably just for storing the cartridge serial number, maybe assay configuration parameters so the device can work offline with new tests.
I think that’s a ceramic heater under the swab. So maybe the metal pad in the reader is not a heater but an electromagnet! Maybe this is some sort of magnetic biosensor? Eg. https://pubs.acs.org/doi/10.1021/acssensors.8b00048#
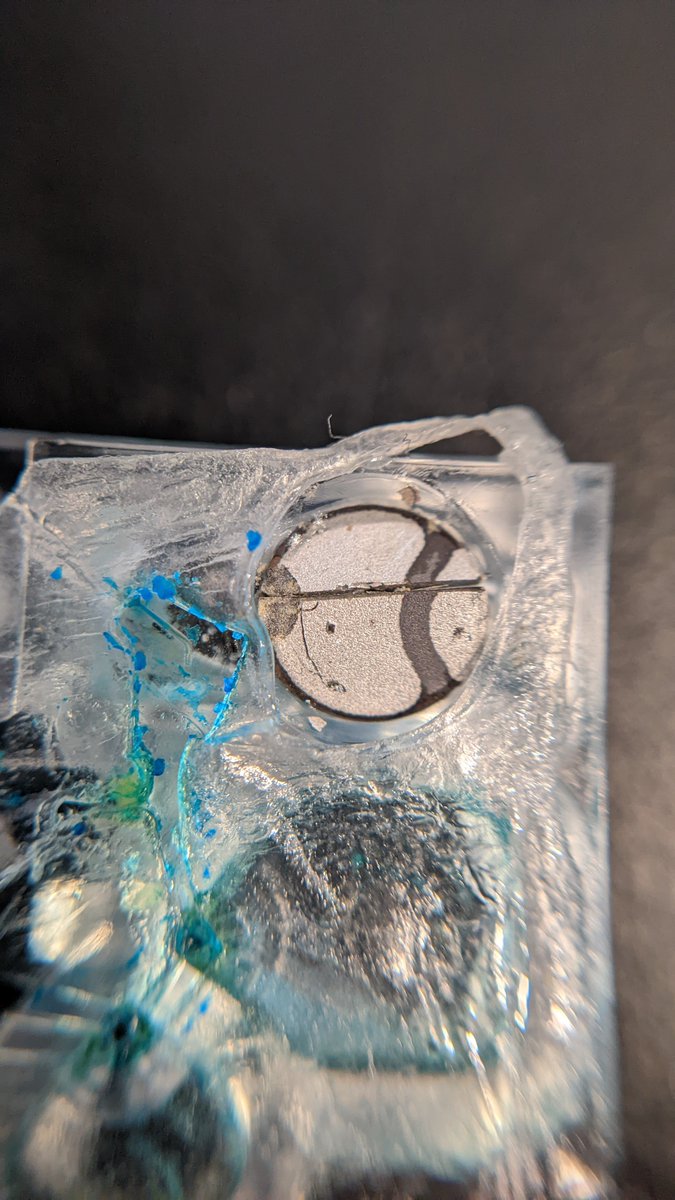

Ah, according to this patent it’s probably a piezoelectric transducer for mixing the sample, not a heater.
Cool! https://patents.google.com/patent/ZA201800856B/en
My wife was asked at the grocery store checkout if she’d like some free rapid tests and the clerk was clearly disappointed when she said “no thanks”. 🙂
My wife explained that we have purchased lots and want to make sure there’s enough tax-funded tests for those less privileged.
According to the clerk, most people are glad to take them and the store has plenty of supply available. Can it be that we’ve nearly reached the elusive goal of universal access to rapid tests in Ontario? 🎉 @C19TestFinders
A great pragmatic workplace screening program, successfully at scale:
RATs used: 321,905
Organizations: 73
True positives: 473
False positives: 75 https://x.com/DavidJuncker/status/1499845986876899331
In this pre-omicron program it would have cost about $4,000 in tests to catch one case and avoid the downstream transmissions. How should we, as a society, decide what the threshold for a good ROI is?
“Everybody wants the pandemic to be over. Everyone. But no more can I wish away winter by wearing flip-flops and T-shirt outside, can I wish away a pandemic by changing what I wear”
Great analogy! https://www.therecord.com/news/waterloo-region/2022/03/11/waterloo-region-district-school-board-rescinds-mask-rule.html
I got my 12yo boosted today despite being a little shy of the 6 month interval. The clinic didn’t even mention the 6 month interval.
With kids back at school without mask mandates next week, the risk tradeoff seems pretty damn clear to me. I’m glad I didn’t have to fight for it.
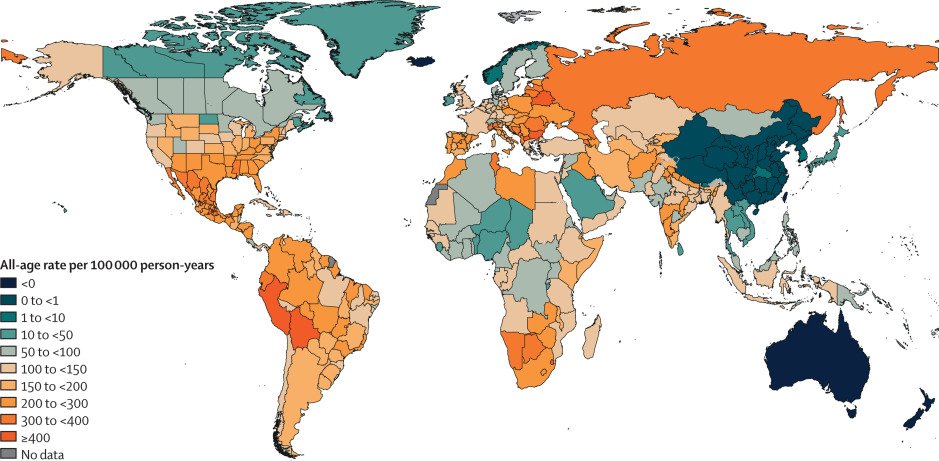
Nice picture summarizing excess mortality from COVID. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02796-3/fulltext
Can you imagine a future where colds and flus are as rare as Cholera and Dysentery today? Will we look back on our evolving treatment of indoor air as we now look back on the treatment of drinking water 150 years ago? https://x.com/joeyfox85/status/1504593227629965314
My son’s report from the first day of grade 10 without mask mandates:
“In business class 20% of the kids were wearing masks. In pre-AP math class it was 80%”
🤔
Also there was a significant decrease in mask wearing throughout the day, with math class being a huge outlier at the end of the day.
A COVID transmission anecdote and live test of my family’s airborne transmission precautions:
My son’s teenage friend rides in a car for ~30 min, masked the whole time. The next day the driver tests positive. Teen is triple vaxxed.
At day two and three post exposure the teen has a negative rapid antigen test. They had plans to come to our house Sunday (with everyone present doing rapid tests) but given the exposure I ask to postpone. Rapid tests aren’t perfect!
Around four days post exposure the teen has a negative PCR test. That’s gotta mean the risk is low, right?
Being masked, the exposure doesn’t count as a “close contact” so the teen is still at school with my son.
Seven days post exposure the teen does another rapid antigen test and this time it’s positive! No symptoms yet.
My son has been sitting next to the teen and eating lunch with them for the past three days. What’s the probability my son is now infected?
Well, my son has made some key decisions (his, not mine):
- Got boosted the first day he was eligible, 6 weeks ago
- Always wears an N95 mask at school
- Eats lunch outside, keeping >1m distant from others (even in our record cold temps, which my wife and I said was nuts).
I figure he’s got a pretty good shot at having protected himself, but with such prolonged exposure the risk has still got to be significant.
My son will be doing rapid tests daily to help reduce the risk of him spreading it to someone else at school. The first is negative.
My son had another negative rapid antigen test and this morning a negative rapid molecular test (Lucira check-it).
For the record, my son continued to test negative on daily RATs. We stopped regular testing about 4 days after end of symptoms (though I admit to testing only every other day during those 4 days). We also just did an antibody test and saw no hint of IgM (only IgG from vaccine).
We’ve been trained to see symptoms as an indicator of contagiousness. For vaccinated people with omicron this appears WRONG. Contagiousness likely follows symptoms. https://x.com/joshgans/status/1511328793063043074
One year ago today we launched the StaySafe community rapid testing program to try to raise awareness of the power of rapid testing in Canada: https://www.canada.ca/en/health-canada/news/2021/04/government-of-canada-invests-in-staysafe-rapid-screening-program-in-waterloo-region.html
Then about 6 months ago the Ontario government shut us down for allowing citizens to access taxpayer-funded tests even when their employer chose not to participate. https://www.theglobeandmail.com/canada/article-ontario-tells-agencies-covid-19-rapid-tests-are-only-for-workplaces/
Cool @miniPCR now sells a COVID testing lab (for educational purposes only): https://www.minipcr.com/product/covid-qpcr/.
Near the start of the pandemic I argued they should do this, so had a hell of a time ordering my own SARS-CoV-2 primers and probes. 1/2
I suspect most everyone was afraid of policy and PR implications of selling SARS-CoV-2 PCR kits to the public. That @miniPCR is now OK doing this signals to me a real opening up of legitimate citizen science. Next up: all respiratory viruses?
Srsly, what are we afraid of? 🙂 2/2
To be fair, companies like @biomeme and @chaibio were already ahead of the game at the start of the pandemic. But selling devices and kits targetted at (and priced for) the highschool classroom is a step function increase in scale and acceptance.
UPDATE: Looks like I spoke too soon. Digging deeper into the instructions I see this isn’t a real virus test kit (no RNA extraction, no reverse-transcriptase). It comes with DNA samples, presumably synthetic. That’s a shame 😢.
We’re already experimenting with COVID transmission in pretty much every single classroom in North America and Europe. Would it really be any more risk to at least get some science education out of it? 😁
Hey @COVIDSciOntario, love your dashboard but isn’t it time to add a “with booster in past 6 months” vaccine effectiveness chart? “At least 2 doses” is now <80% protective against ICU and falling! https://covid19-sciencetable.ca/ontario-dashboard/#riskbyvaccinationstatus
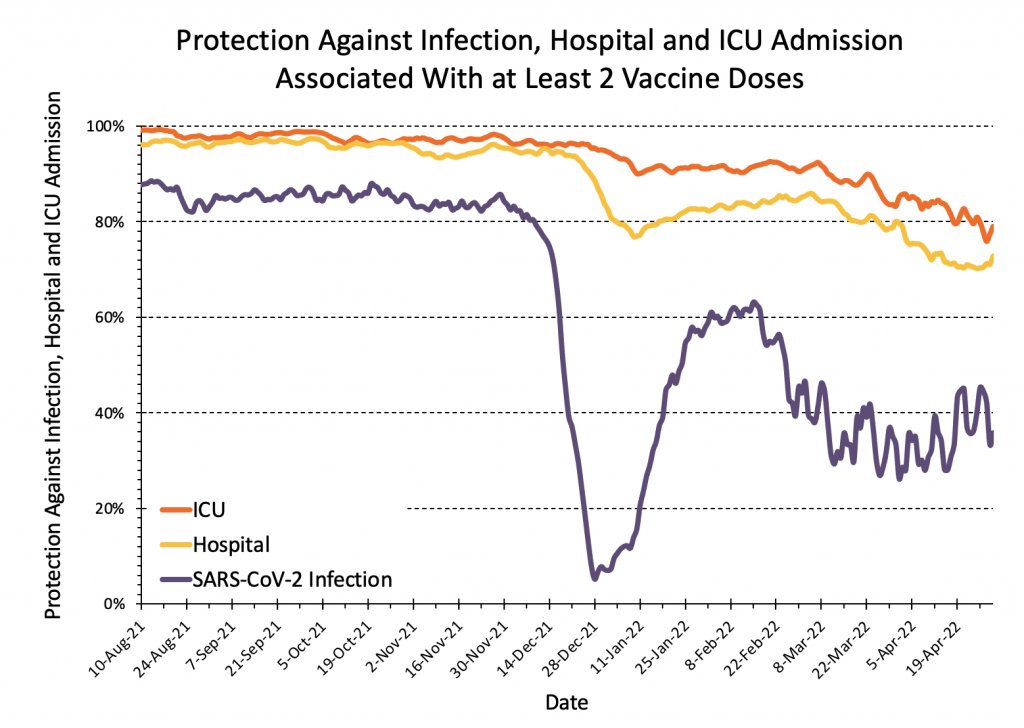
These graphs did an excellent job explaining the value of vaccination to Ontarians right up until December. Now they’re really failing to capture the most valuable opportunity. What gives?
“How do we make vaccines that are good at completely stopping infection with respiratory viruses? We need to solve that problem as soon as we possibly can.”
Yes! Why aren’t more experts seriously asking this question?
https://www.theguardian.com/society/2022/may/05/are-nasal-sprays-vaccine-answer-to-stopping-covid-transmission
I wonder how many other pandemics we’ve narrowly avoided by one of the first transmissions being interrupted somehow?
What small thing would it have taken to prevent these last two and a half years of hell?
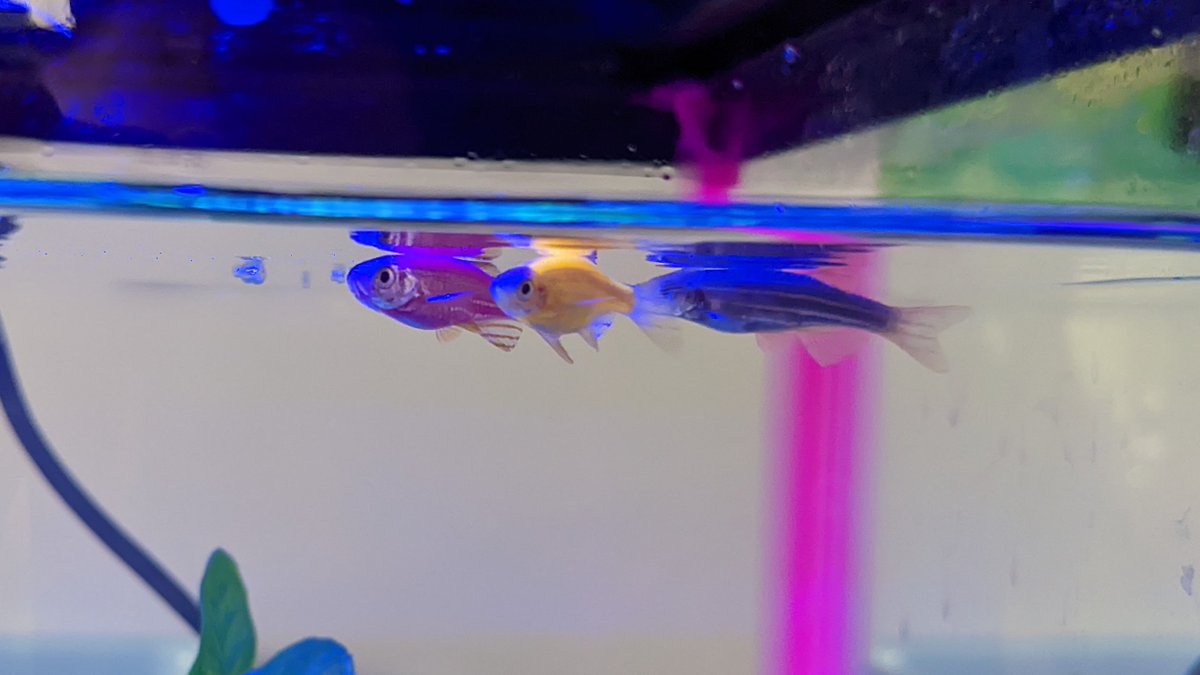
My daughter got some new pets today: genetically engineered Tetra GloFish®️
https://en.wikipedia.org/wiki/GloFish
What excites me is not that these exist (standard lab work these days), but that PetSmart has a whole wall of them and people are by-and-large cool with it! 🤓
This certainly beats the home CRISPR kit we were planning on trying on bacteria: https://www.the-odin.com/diy-crispr-kit/.
I’m picturing what PetSmart might look like in 20 years. Are we at the dawn of a modern “Cambrian Explosion” in biodiversity? Yes, gotta be mindful of ethics and safety.
Protection from hospitalization by vaccination continues to fall, now below 70% in Ontario! That’s >6x worse than 6 months ago! To what extent is this due to low uptake of boosters, boosters waning, or continued mutation? @COVIDSciOntario
https://covid19-sciencetable.ca/ontario-dashboard/#riskbyvaccinationstatus
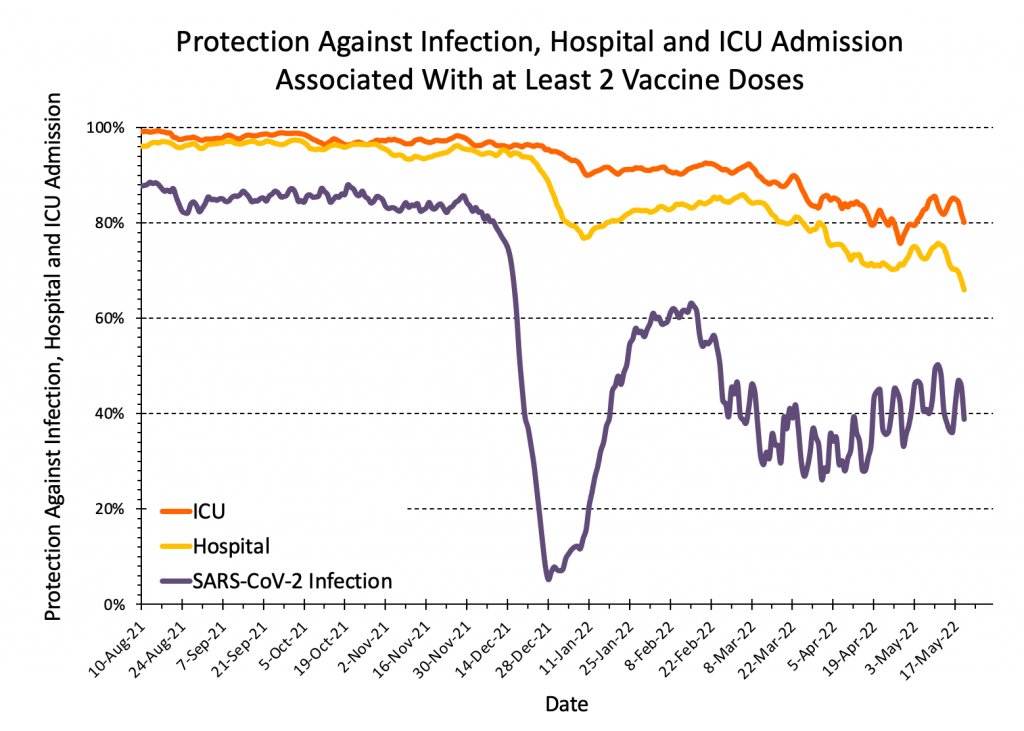
At this point, isn’t this the MOST important indicator for the impact of the pandemic? Why aren’t more people talking about it and pushing to figure out how to get us back to >95%? @imgrund @DFisman
Well crap, this is frightening. 2 doses of vaccine seem to do nothing to reduce the risk of long term neurological issues from COVID (but of course does reduce the risk of death). Hopefully we’ll learn a booster helps. Until then, I’ll keep my N95 on!
https://www.nature.com/articles/s41591-022-01840-0
Prediction: 5 years from now when the impact is undeniably obvious, everyone will complain: why didn’t healthcare experts warn us of the risks of long COVID and explain how a simple N95 could massively reduce our risk without lockdowns?
Finally! Vaccine manufacturers are starting to make noise about providing better protection against Omicron: https://investors.modernatx.com/news/news-details/2022/Moderna-Announces-Omicron-Containing-Bivalent-Booster-Candidate-mRNA-1273.214-Demonstrates-Superior-Antibody-Response-Against-Omicron/default.aspx
Common science, you need to move a LOT faster! 💉💨@RADVACproject
I couldn’t keep asking my son to miss life experiences, so I took him to paleontology camp in the US.
Pro: 3 awesome days of learning from paleontologists in the field.
Con: COVID+ on day 4, now stuck in a hotel in the middle of nowhere for at least 10 days 😥.


This is huge! It means we might just have a shot at catching up with this thing! Please Health Canada, don’t move any slower than the FDA! 🙏https://www.theverge.com/2022/7/1/23191165/covid-variant-trials-vaccine-booster-fda
It’s crazy that antigen tests are available in most pharmacies in the US yet only in one or two packs!
I order boxes of 25 at home, and Ontario gives out 5 packs in grocery stores. Buying in the US feels like such a waste of packaging, not to mention higher prices!
Clear and accurate message with great visuals! Public health agencies take note! https://x.com/JohnSnowProject/status/1546245019702640641
Despite our best safety efforts, my son and I got COVID while travelling in the US. We both qualified for Paxlovid and it worked extremely well except that I had a rebound. Here’s a visual representation of the progression with RAT images. https://docs.google.com/spreadsheets/d/1FcPSet0gHpoW9WQ4GTBCdV7brnDfEOC5fRTTvx4-mBQ/edit?usp=sharing
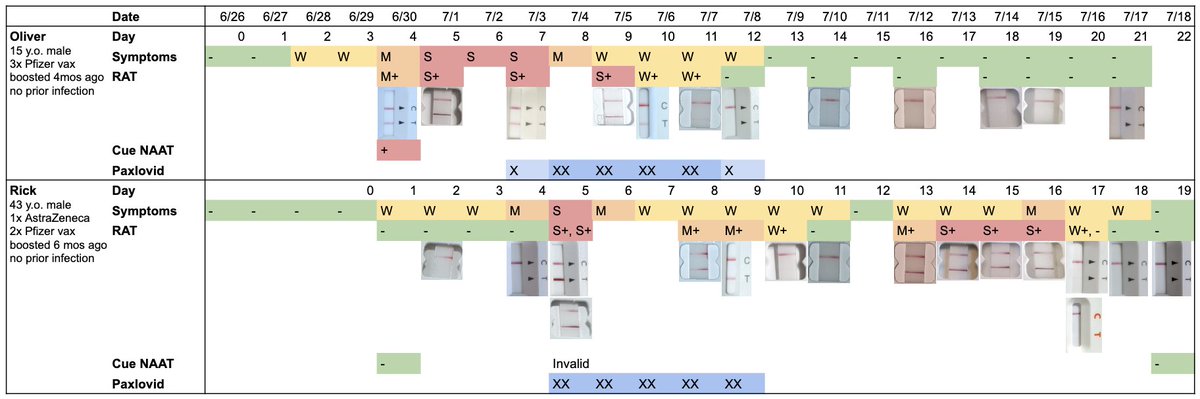
I researched Paxlovid in some detail in advance and saw the trials showed a <2% risk of rebound, same as placebo. But I regret not searching Twitter, as if I had seen this I would have delayed starting my treatment a couple days post symptom onset. https://x.com/michaelmina_lab/status/1521249046425440258
I’m sad that when COVID finally caught up with me, I was away from my lab and so couldn’t collect daily samples for PCR Ct monitoring. I did collect one sample near the end, I’m hoping to figure out how to get it sequenced so I can see where we fell on https://nextstrain.org/ncov/gisaid/global/6m.
I am optimistic that some of Canada’s public health agencies have learned from COVID diagnostics and surveillance and will apply those learnings to Monkeypox. Sadly I haven’t seen any evidence yet, anyone else? https://x.com/michaelmina_lab/status/1556094734849949697
@GovCanHealth did exactly this for COVID. How long do we have to wait until we get it for MPV too? I can buy a home HIV test in Canada, why not a Monkeypox test? https://shop.insti.com/insti-hiv-self-test https://x.com/RanuDhillon/status/1556937507786219520
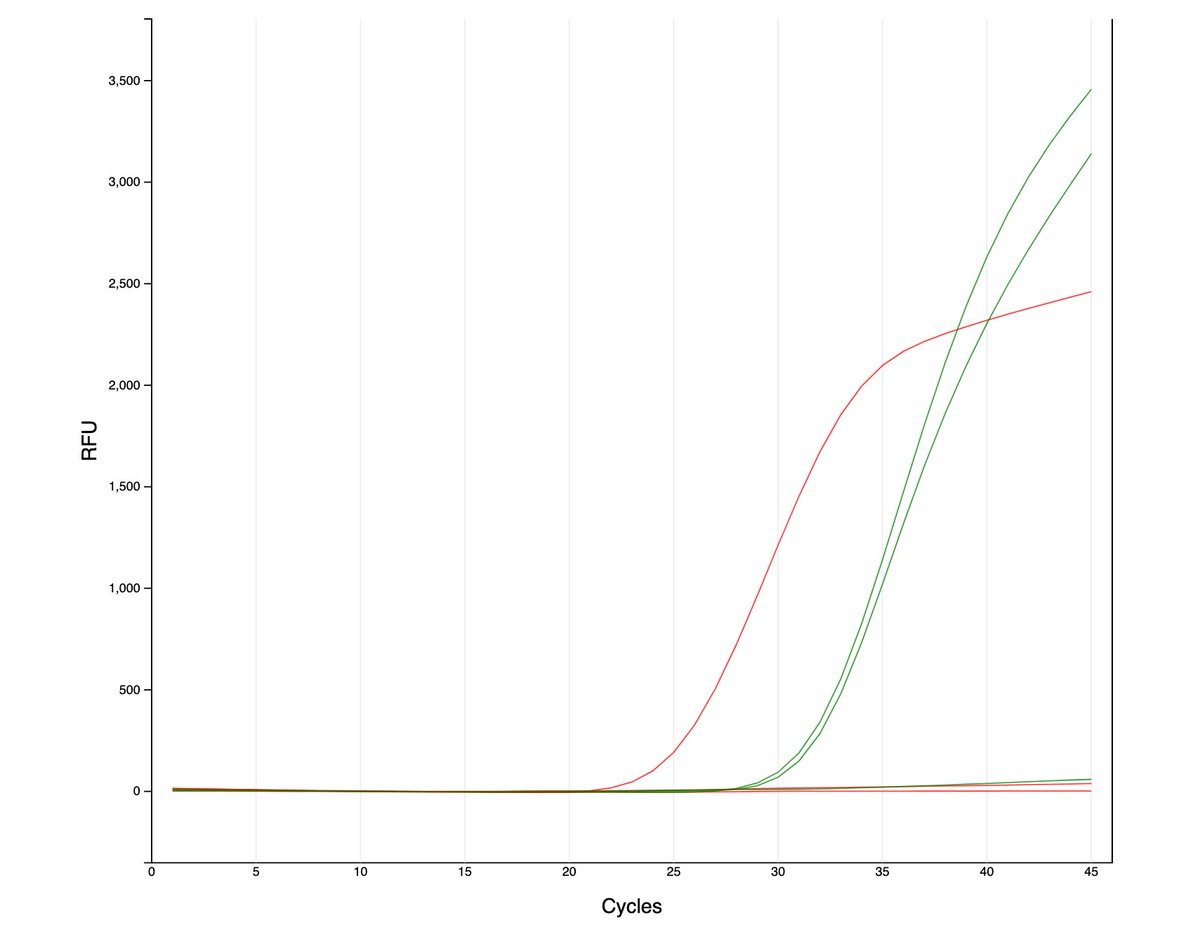
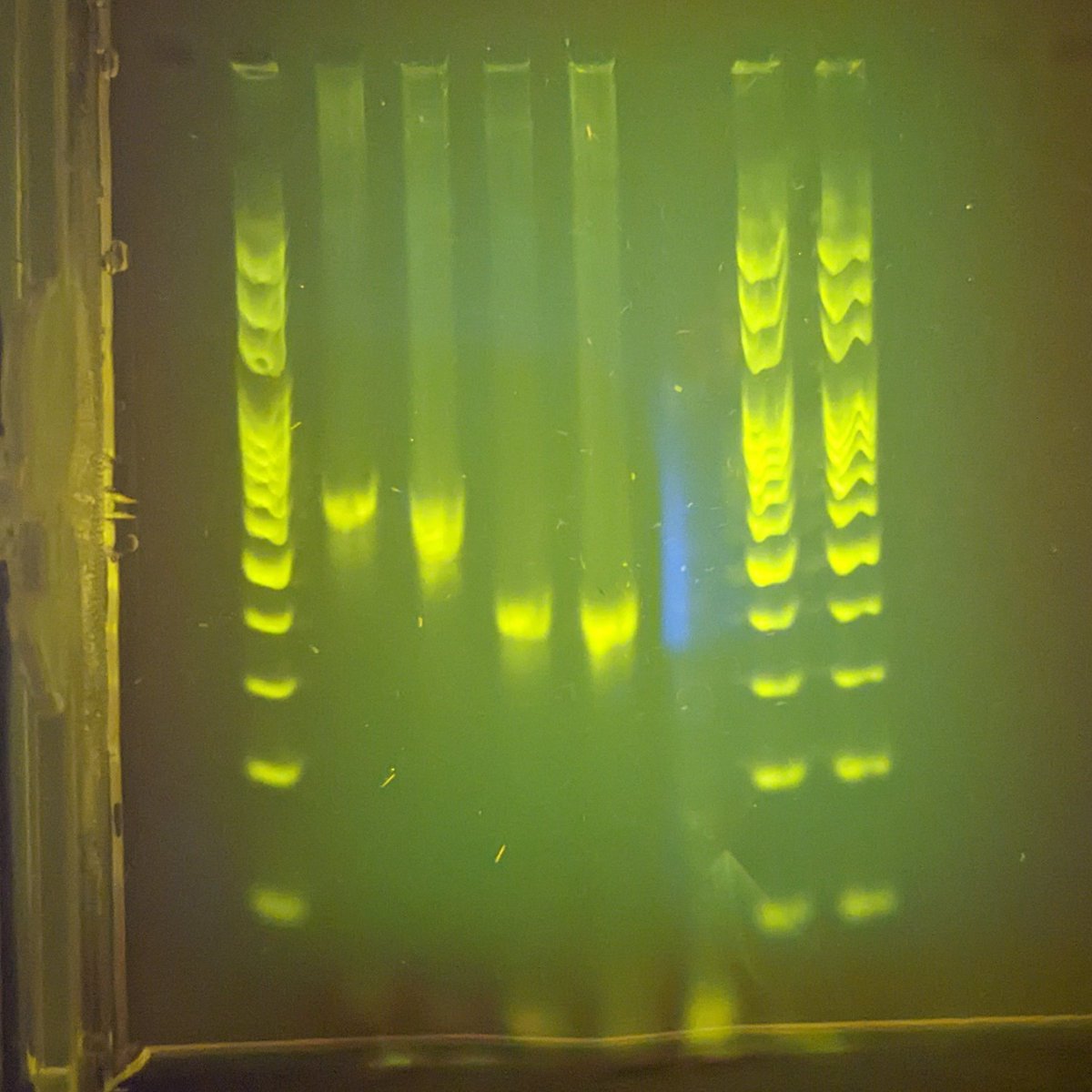
Finally got around to running qPCR on my personal COVID sample taken on my last day of antigen positivity.
Ct of 29 on CDC N1 and N2 targets (green lines, red is internal control, 3rd sample is negative control).
Next step: figure out sequencing and variant analysis!
Fascinating to see the progression of COVID by RNA copy number, viral load (culture) and Innova RAT result across a variety of individuals:
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(22)00226-0/fulltext.
This paper has several surprises for me: 1/6
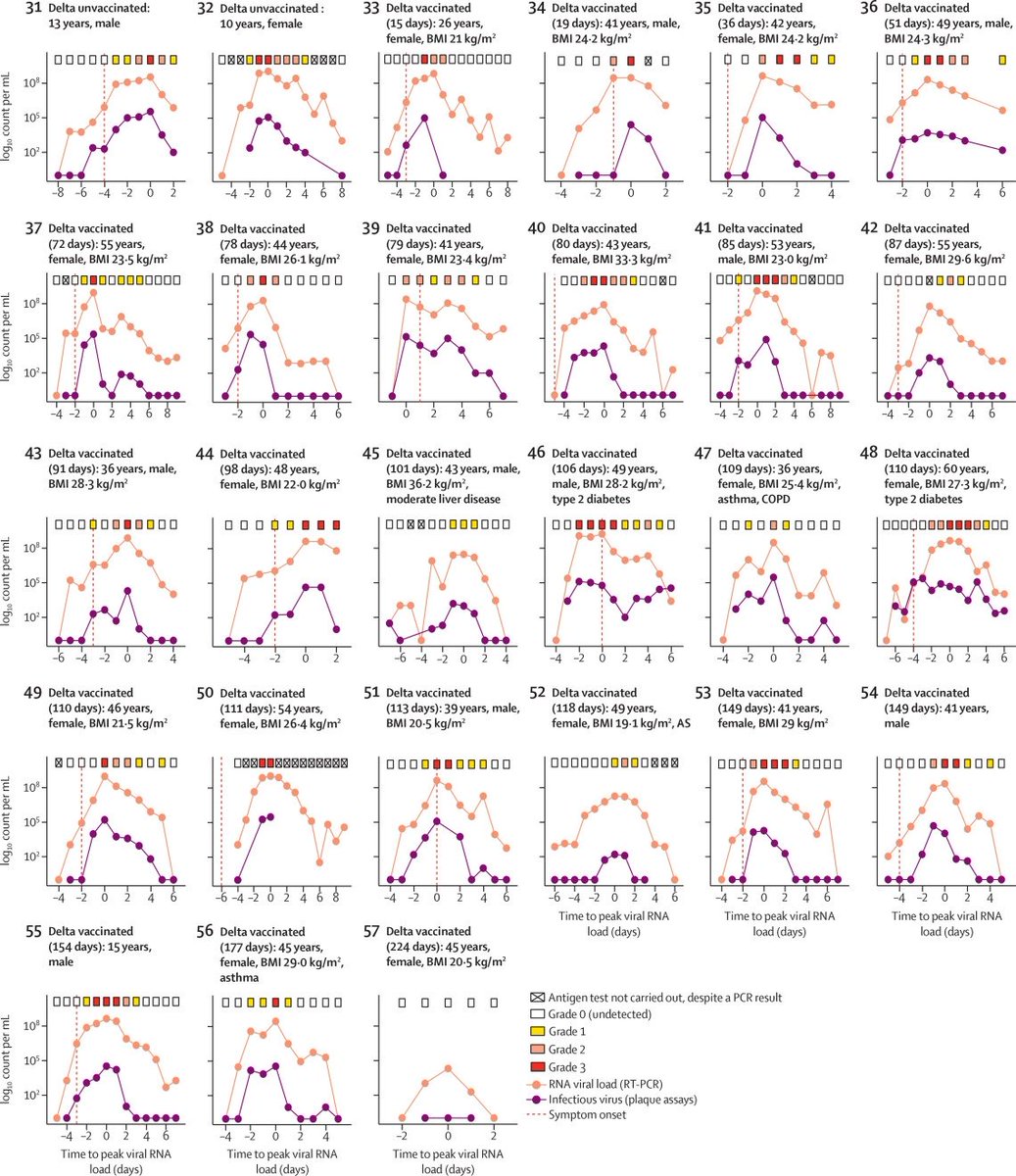
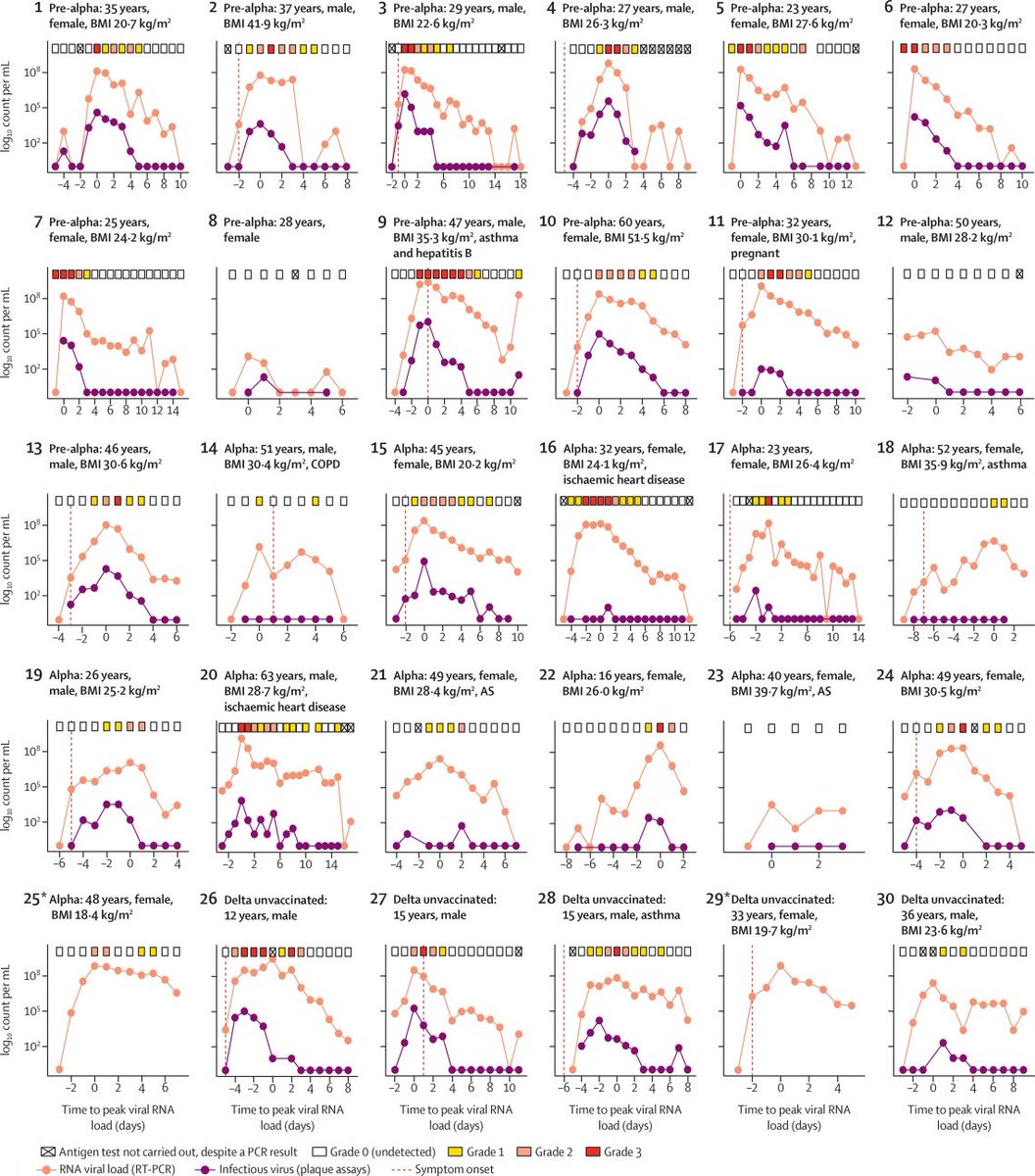
Only 6% of cases were asymptomatic and only 25% shed culturable virus pre-symptomatically. This is a pre-omicron largely unvaccinated population, but from earlier studies I’d expect ~50%. 2/6
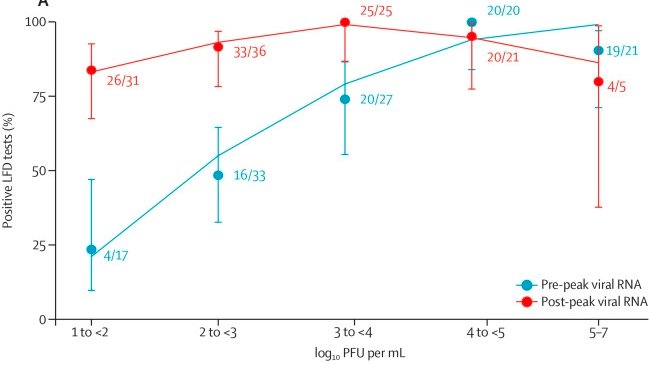
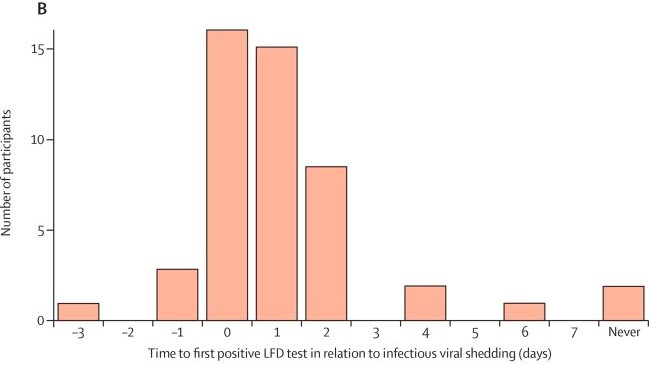
As expected, RAT sensitivity correlated with viral load. However this correlation disappeared in the period after peak viral RNA! 3/6
There were a few more instances of culturable virus with negative RAT than I would have hoped or predicted. The paper calls these “infectious”, but as @profvrr likes to remind us: “culturability doesn’t necessarily imply infectiousness”. 4/6
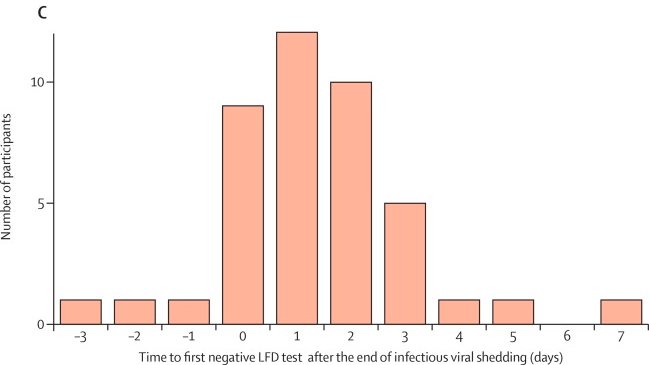
There were more cases of positive RAT days after virus was no longer culturable than I would have expected. 5/6
We all know RATs are imperfect and it’s informative to see some better details quantifying that imperfection. But this study largely confirms the argument of @michaelmina_lab and others that frequent rapid antigen testing is the best practical way to predict contagiousness. 6/6
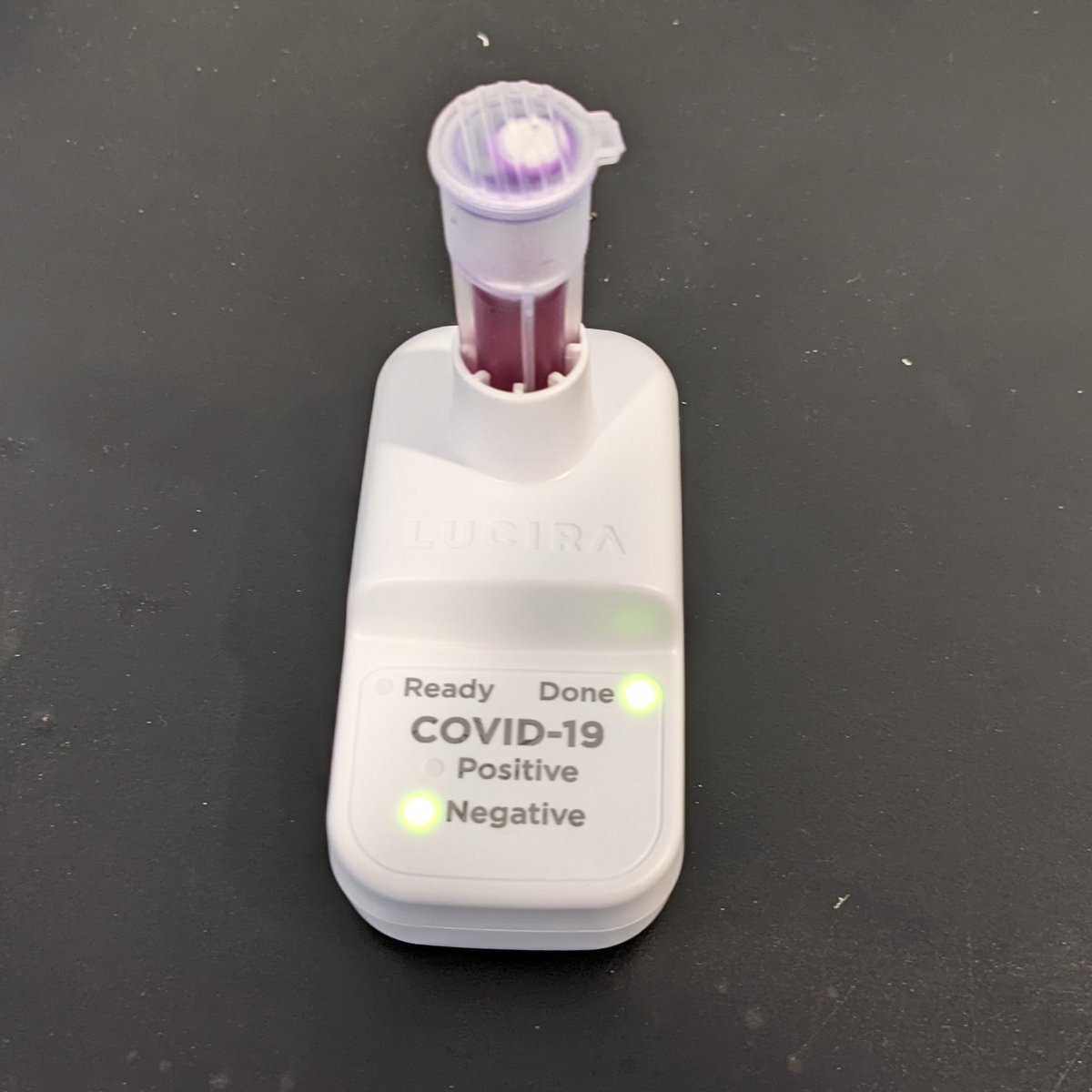
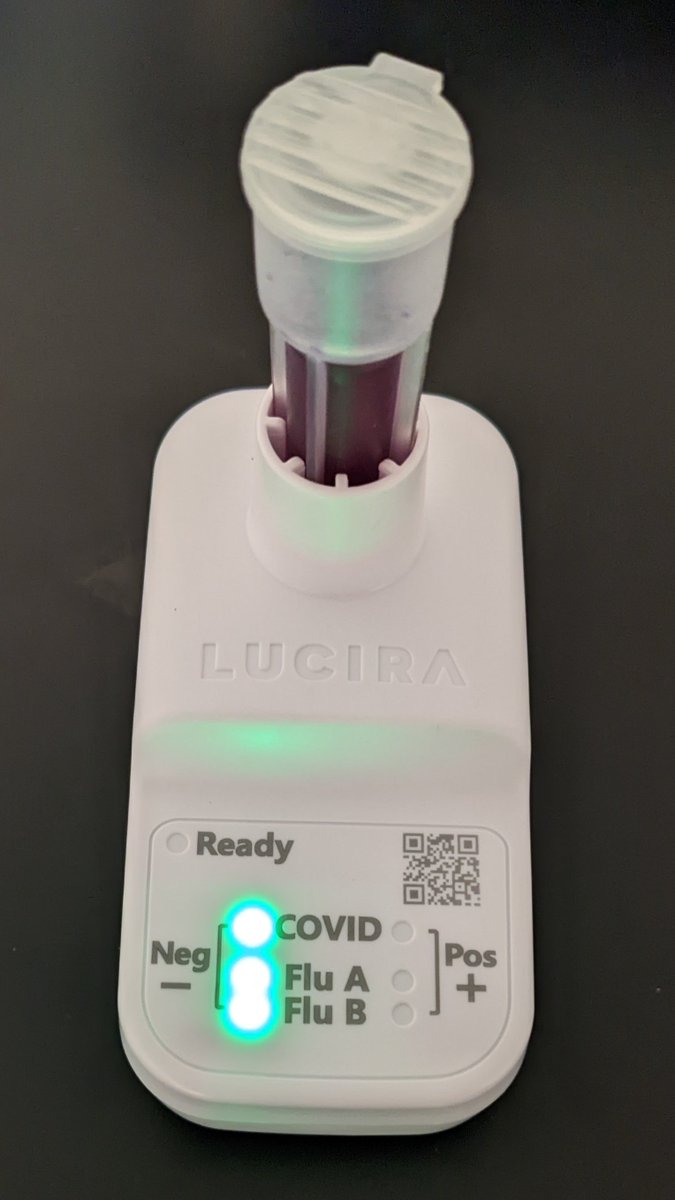
I just learned @LuciraHealth has a home COVID+Flu test on the market in Canada. This is great, another step towards easily being able to identify any common infection at home! Ordered! https://checkit.lucirahealth.ca/products/lucira-covid-19-flu-test
For my birthday my kids got me some supplies for my molecular biology lab. I’m not sure if I should be offended or proud 😛.
In case it’s not obvious, for the record the shirt is a joke and I do indeed take lab safety seriously.
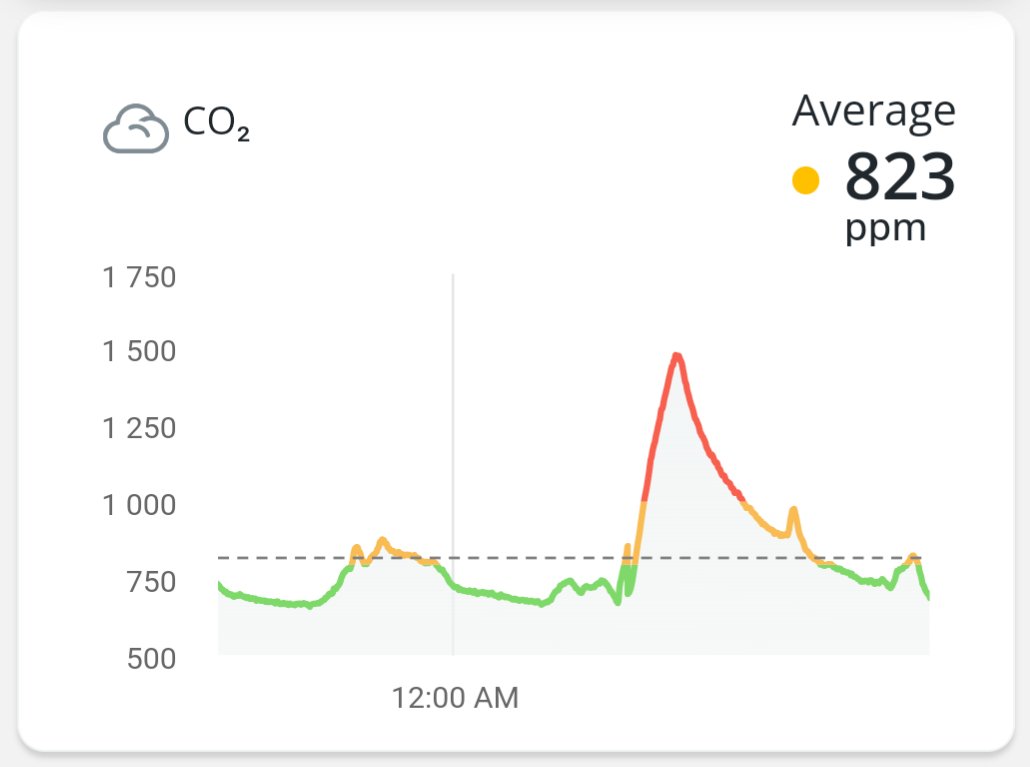
Had a dozen friends over, CO2 really spiked! This is in a large house with an air exchanger on medium, measuring with @airthings in an unused room.
It’s a good reminder of how much we’re breathing each other’s air even when 6 feet apart! In this case, everyone did COVID RATs.
Direct sequencing in a toothbrush. 🤯
The future will be incredible and here faster than you think! https://x.com/nanopore/status/1527352356622389250
Got a new piece of lab equipment, a magnetic separation rack for DNA purification! 😁
But something seems messed up with the market when the cheapest version, some plastic and three rare earth magnets, costs $300! 😂
https://www.neb.ca/detail.php?id=7017
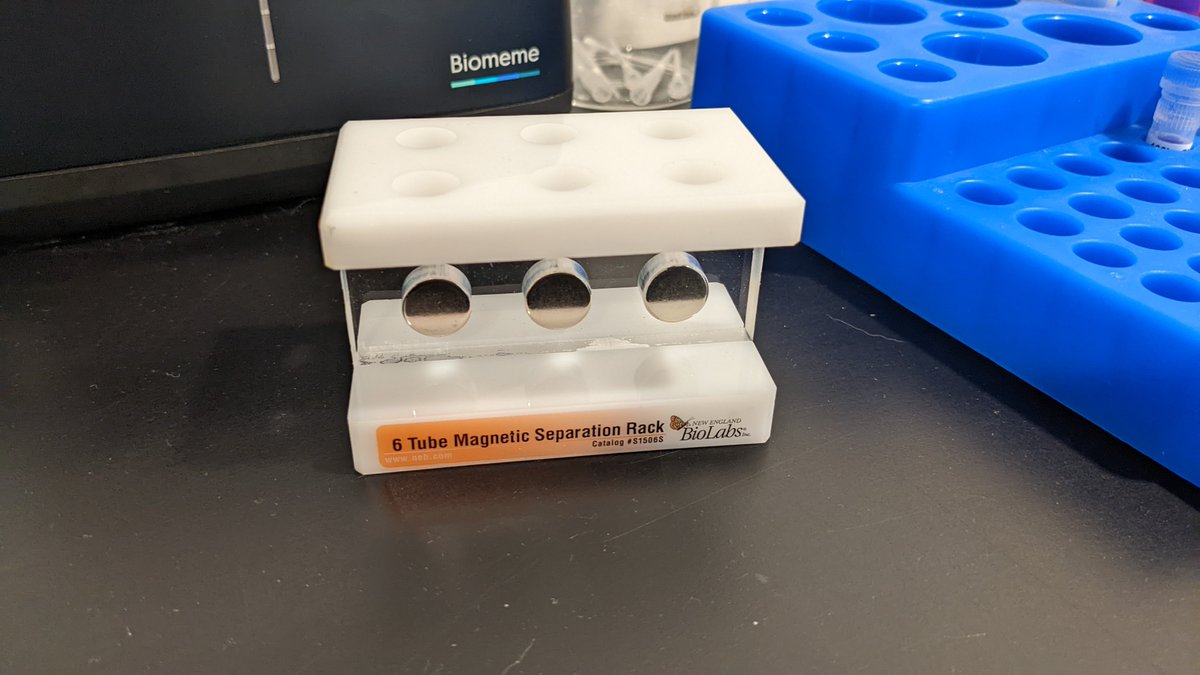
Looks like I should have searched Etsy or just made it myself! 🤣

I attended a week-long conference with ~400 people. Every single one of us did a rapid test every morning and wore a mask when indoors (almost all N95). Many of us ate only outdoors. It really wasn’t hard at all and worth it to see people IRL! https://www.w3.org/2022/09/TPAC/health.html
I, and many others, would have still attended with fewer rules. I’m sure many felt it was overkill for them personally. But we all knew someone at higher risk and so we were happy to take extra precautions to be as inclusive as possible.
Also the organizers did an awesome job ensuring people could participate in every meeting remotely. Being in person was better, but being engaged was possible regardless of willingness to travel.
Been waiting for a study like this! Cutting long-COVID risk in half is good news. Let’s hope that variant-matched boosters cut it much further than that! https://x.com/DFisman/status/1570901408211402752

The future is finally here!
In the past week I’ve gotten two technologies I’ve dreamed of owning for a decade: a self-driving car and a genome sequencer.

Neither is actually practical for widespread consumer usage yet. But the remaining journey now seems imminent and inevitable rather than being science-fiction.
My first multiplex consumer molecular viral test is all clear. 🎉
This @LuciraHealth “Check It” isn’t nearly as powerful as my 15-virus home qPCR panel, nor as cheap on a per-sample basis ($75 vs. $20). But being simple to use makes it way better! https://x.com/RickByersLab/status/1562466594684829702
Yesterday I hit my pre-decided conditions for ending my strict mask wearing at work.
Today someone I spent a bunch of time in a small meeting room with told me they tested strongly positive.🤦♂️
Great to see the FDA expanding their requirement for serial testing using antigen tests. https://www.fda.gov/medical-devices/safety-communications/home-covid-19-antigen-tests-take-steps-reduce-your-risk-false-negative-fda-safety-communication
Some things still seem quite confused here though: 🧵 [1/10]
Guidelines to test 3 times over 4 days makes a lot of sense. Hopefully this will result in more useful test packaging in the US. https://x.com/RickByersLab/status/1545531974776983553
But what is the guideline on when to START testing after exposure? After infection, the virus “latent” (replicating but not shedding) for the first 2-3 days, maybe up to a week or more. Testing on only day 0, 2 and 4 after exposure would give a dangerous false sense of security!
The cited study does a great job of tracking individuals over time and excluding those with prior infection in order to focus just on the onset of infection (avoiding the all-too-common post-contagious-period bias in similar studies). https://www.medrxiv.org/content/10.1101/2022.08.05.22278466v1.full
But it treats “is currently infected” as the only data point of value, perpetuating the terrible idea that home use tests are for “detecting an infection” rather than the public health goal of minimizing the risk of onward transmission. In contrast see: https://x.com/RickByersLab/status/1561470940109733890.
What does the FDA even mean when they say “infected”? Eg. they say “Molecular COVID-19 tests are generally expected to detect the SARS-CoV-2 virus at least 95% of the time when someone is infected”. But with a latent period of >2 days, this is likely mathematically impossible!
I think maybe when the FDA says “infected” they mean “shedding RNA as detectable by PCR”, a circular definition! This is what has led to all the confusing and flawed reasoning evaluating antigen tests that @michaelmina_lab has been fighting against for years.
The overall message still reads like antigen tests have poor performance (especially for asymptomatic people) while lab PCR tests are perfect. Why doesn’t anyone talk about all the false negatives that occur in lab PCR tests performed during the unpredictable latent period?
The message should be: “Since there is variability in time from exposure to becoming contagious and since no test is perfect, repeat testing over days 3-7 after exposure is necessary in order to conclude an individual is not likely to become contagious.”
And also “Testing after the onset of symptoms or with a molecular test (instead of an antigen test) can help reduce this window of uncertainty by a day or two, but not eliminate it.” [10/10]
My first run on a minION sequencer. If all goes to plan, later today I’ll have the sequence of the SARS-CoV-2 virus that infected me!
24 million bases called in less than 30 min, should be more than enough for a 30kb genome!
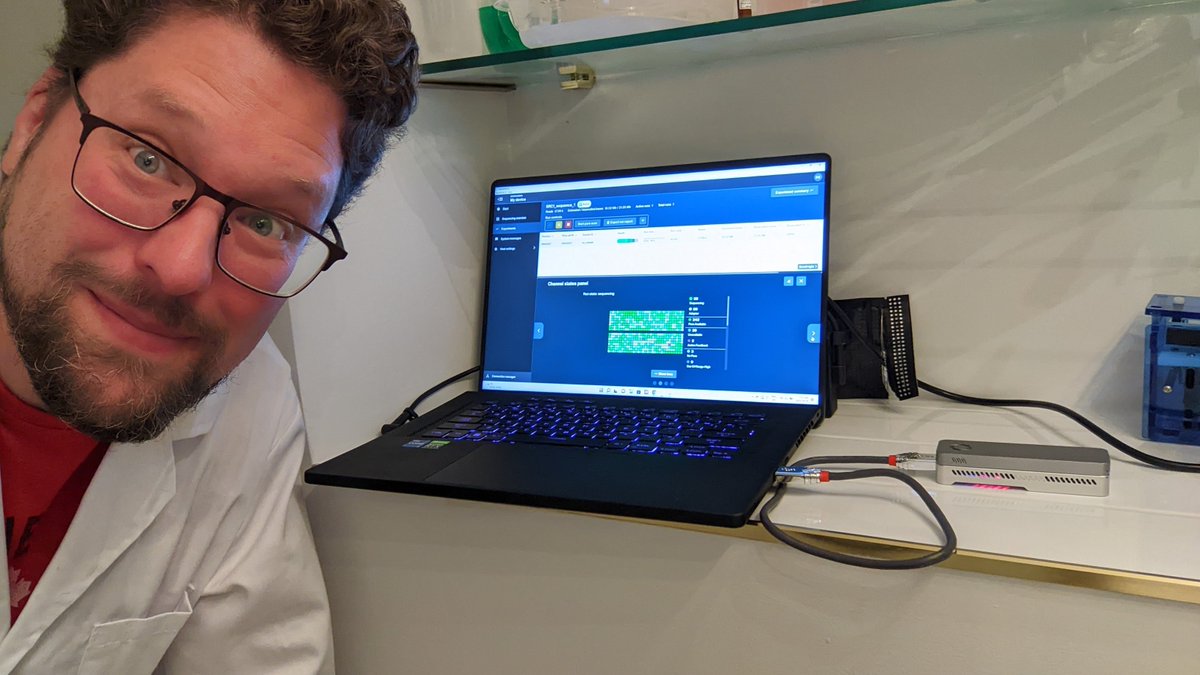
It looks like I had BA.5.2.1.
Here’s a screenshot of some reads showing a A->G mutation at 27038, one of the defining mutations of the BA.5.2.1 lineage: https://github.com/cov-lineages/pango-designation/issues/657

Correction: using a more recent Nextstrain it more precisely classified my virus as BF.28, aka. BA.5.2.1.28.
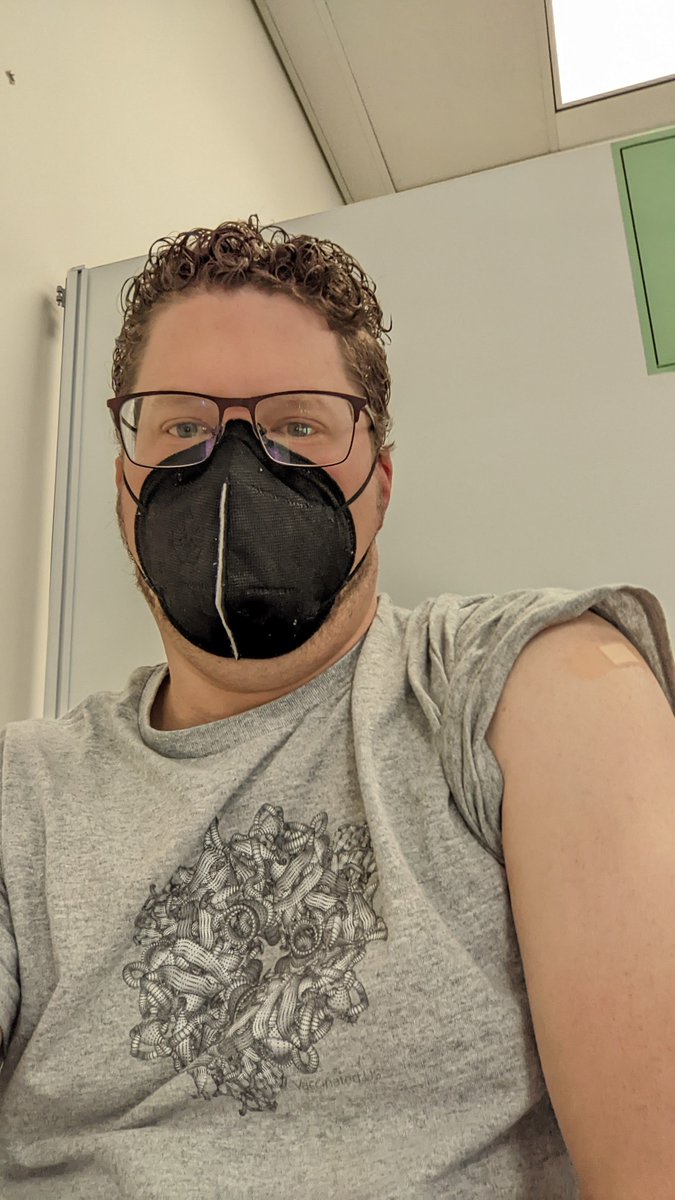
Wore my @VaccinatedUS shirt to get my @pfizer bivalent BA.4/5 booster this morning. It turned out it was a new @ROWPublicHealth clinic and I was their very first customer! 🎉
The doctor was surprised that a software engineer had been able to sequence their own SARS-CoV-2 genome🤓
Great to finally see data on this! Though I guessed the effect would be much stronger. My hunch that this would be true is why I got Paxlovid for my son and I when we had COVID in July. We each have one minor risk of progression. https://x.com/VirusesImmunity/status/1589421635257663489
Interesting… Is this dangling new money carrot under conditions of more data sharing and interoperability across the country? If so, I think like it! 🙂 https://x.com/jyduclos/status/1589776091144925184
I asked @midjourney_ai to imagine me working in my lab. Here are some of my favourites. 🤯



Not exactly accurate 😂. But just imagine the power of AI-generated imagery for science communication if the accuracy continues to improve at it’s current pace and tools build the ability to refine specific details.
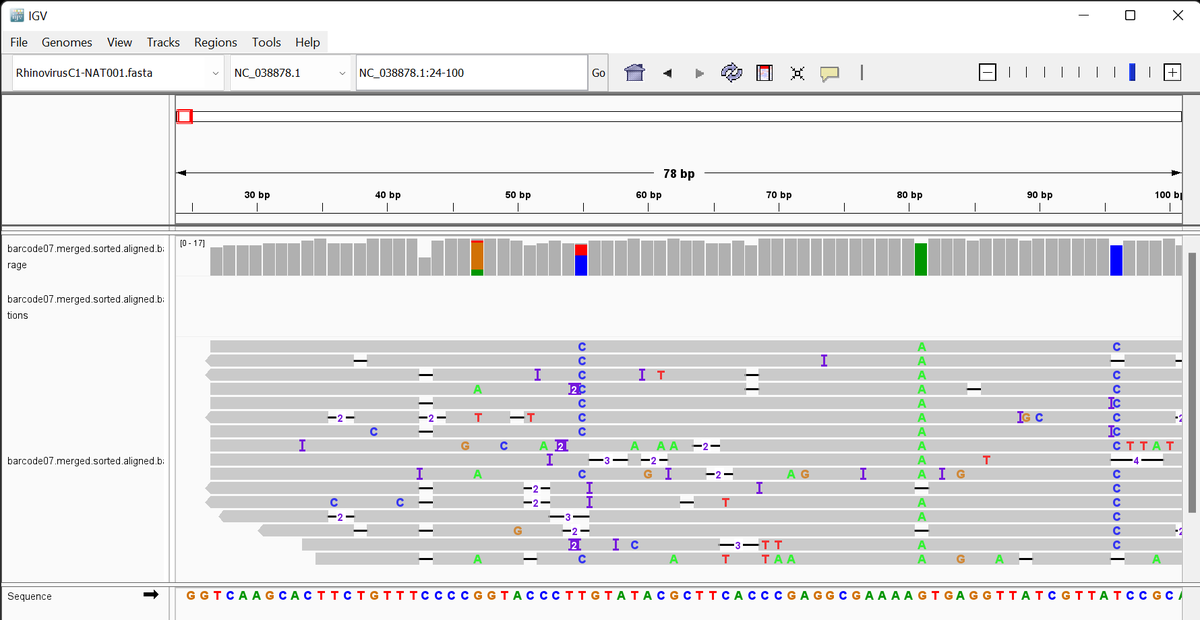
My son had a bad cold, but COVID tests were negative so we wondered what it was.🤒🤷
I just sequenced a piece of it and found it was Rhinovirus C, the “NAT001” strain!🧬
Someday this will be trivial and cheap to do at home. Knowledge is power!🧠⚕️

Great video! I am really baffled why this excess mortality data isn’t better known. Thanks for the ongoing investment in education @VaccinatedUS! https://x.com/VaccinatedUS/status/1598811539217293312